Michael Robinowitz M.D. earned his medical degree from Chicago medical school in Chicago Illinois. He completed a residency in gynecology and obstetrics at Emory University school of medicine. Dr. Robinowitz joined Piedmont Fayette Hospital in 2009 as medical director of the Wound Care center and medical director of the hyperbaric services which started in 2012. Prior to joining Piedmont, he was a clinical professor at Emory University school of medicine and attending physician at Grady health systems. At the same time was in practice at Meridian medical group/Prucare of Atlanta where he was chairman of the board of this 60 person physician group. Currently he is a board certified fellow of the American College of OB/GYN, a fellow of the American Professional Wound Care Association, a fellow of the American College of Hyperbaric Medicine and is certified in hyperbaric medicine and wound care.
Robinowitz_Current Dialogues in Wound Management_2017_Volume 3_Issue 1
The patient is a 32-year-old male with history of lymphoma and avascular necrosis of both hips. On July 8, 2015 the patient underwent a left hip replacement done for severe pain due to avascular necrosis. During the procedure the patient lost an excessive amount of blood and required four units of blood postoperatively. The patient was discharged home three days later. Initially he did well but then started noticing weakness, chills, left leg pain, surgical site pain and swelling. On July 17, 2015 the patient went to the emergency department due to worsening anorexia, erythema, edema and tenderness at the surgical site.
Past medical history:
1. Lymphoma in remission
2. Avascular necrosis of both hips
3. Post chemotherapy problems causing organ shut down, kidney failure and myocarditis (2015)
Social history: Former smoker. Denies drugs. Occasional alcohol use.
Family history: A family history of pyoderma gangrenosum (PG) in his paternal aunt after a cesarean section. She spent 60 days in the hospital. After genetic testing his father and uncle were told that they were positive for pyoderma.
Allergies: morphine and remote penicillin allergy. Physical exam on admission: Blood pressure 123/70, pulse 109.and temperature 98.2
Laboratory results and x-rays: White blood cell count 24,100 with 16% bands. ESR was greater than 140 and the CRP was greater than 45. Initial x-ray of the hip showed no acute abnormalities or infectious processes.
Positive physical findings include a left hip surgical wound with marked peri-wound edema, erythema and tenderness. The thigh is swollen. The edges of the wound were open and had signs of necrosis and maceration. No purulence. The incision showed three different ulcerative lesions centered around the incision. The largest ulcer is approximately 3 cm in diameter and is not full thickness.
 Figure 1. July 17th, 2015
Figure 1. July 17th, 2015
The assessment by infectious diseases (ID) and the orthopedist was systemic inflammatory response syndrome most likely related to post-surgical wound infection and possibly pyoderma. The orthopedist and ID physicians were unsure of the specific diagnosis but were treating for both. Wound cultures did not grow bacteria but 1 bottle of 2 blood cultures grew out staph saccharolyticus. The consultant dermatologist was also highly suspicious for PG. The patient chose not to have a biopsy because of the fear that if PG was the cause that a biopsy would cause pathergy and the wound could get worse. On July 24, 2015 the patient was started on a 60 mg prednisone taper because of the pyoderma. A CT scan done on the left hip showed a small fluid collection, and a left hip aspiration was done and sent for culture and sensitivity which came back negative. On July 25, 2015 the patient developed an incomplete left common femoral deep vein thrombosis and started on Xarelto® (Bayer Aktiengeselischaft, XX). Prior to discharge the orthopedist discussed with the patient about the risks, benefits, pros and cons of further surgery to wash out the hip and debride as needed. The patient chose not to have surgery but would continue to be treated for pyoderma by the dermatologist.
The patient was discharged on August 3, 2015 and was sent home on Levaquin, doxycycline and prednisone and given an appointment to the wound clinic. The patient was seen on August 11, 2015 in the wound care clinic. The wound measured 6.2 x 4.2 x 0.1 cm. with a moderate amount of serosanguinous drainage. Subcutaneous tissue was exposed and the peri-wound had blanchable erythema. The patient continued to be seen in the clinic. On September 2, 2015 the patient saw a rheumatologist for evaluation and treatment and was started on colchicine 0.6 mg daily, dapsone 100mg daily (to be started after finishing Bactrim) and prednisone.
 Figure 2. September 11th, 2015
Figure 2. September 11th, 2015
IVIG was started on 09/11/2015. The wound was closed on March 30, 2016 and the patient was discharged from the wound clinic. As of October 15, 2016 the patient is still taking colchicine, Dapsone, prednisone and IVIG and is scheduled to have a total hip replacement in November 2016 and will probably stay on medications until after the surgery.
 Figure 3. October 23rd, 2015
Figure 3. October 23rd, 2015
Pyoderma granulosum(PG) Is an uncommon inflammatory and ulcerative skin disorder characterized histologically by the accumulation of neutrophils in the skin and may occur independently or in association with a variety of systemic diseases such as ulcerative colitis, Crohn’s disease, polyarthritis, gammopathy, vasculitis, leukemia and other conditions. The pathogenesis of PG is multifactorial and involves neutrophilic dysfunction, inflammatory mediators, and a genetic predisposition. PG occurs in about one and 100,000 persons each year in the United States. It affects both sexes but a slight female predominance may exist. It may occur in all ages but predominantly occurs in the fourth and fifth decades of life. Prolonged treatment is often necessary for some patients. Follow-up studies of patients with PG suggest that with treatment more than 50% of patients achieve complete wound healing within one year. It took 10 months for our patient’s wound to heal. Other key names for PG include postoperative PG, post-surgical PG (PSPG), pathologic pyoderma and superficial granulomatous pyoderma. The most common presentation of PSPG is the rapid development of one or more painful purulent ulcers with undermined borders on sites of normal or traumatized skin such as an operative site.
 Figure 4. December 27th, 2015
Figure 4. December 27th, 2015
The vast majority of cases occurred at the surgical site, but in several cases PG also developed at distant locations such as IV puncture sites on the arms and on the shins after breast surgery. PSPG has a few characteristics different than non-surgical PG. In a study of 136 patients with PSPG done by the mayo clinic, 90 (66%) did not have associated systemic diseases as compared to 50% of non PSPG patients. Predisposing risk factors for developing PSPG include: a prior history of confirmed or suspected PG, inflammatory bowel disease, Rheumatoid arthritis, leukemia, lymphoma or myelofibrosis and a family history of pyoderma. In PSPG having had breast surgery, appearance of discrete wounds involving multiple surgical sites that surround but spare the nipple should raise suspicion for PG rather than an infection or ischemia. As in our case presentation it can occur after minor trauma or surgery and has been reported after many different types of surgical procedures. Recognition post operatively may be difficult as it is often misdiagnosed as a wound infection. Early recognition of PG is important as pathergy may occur when debridement is done as when treating what is thought to be a typical necrotic infected postoperative wound diseases. If a comorbidity was present hematologic disorders were most common. 29%(28) of women had predisposing disease versus 53%(19) of men. This too is different than NSPG.
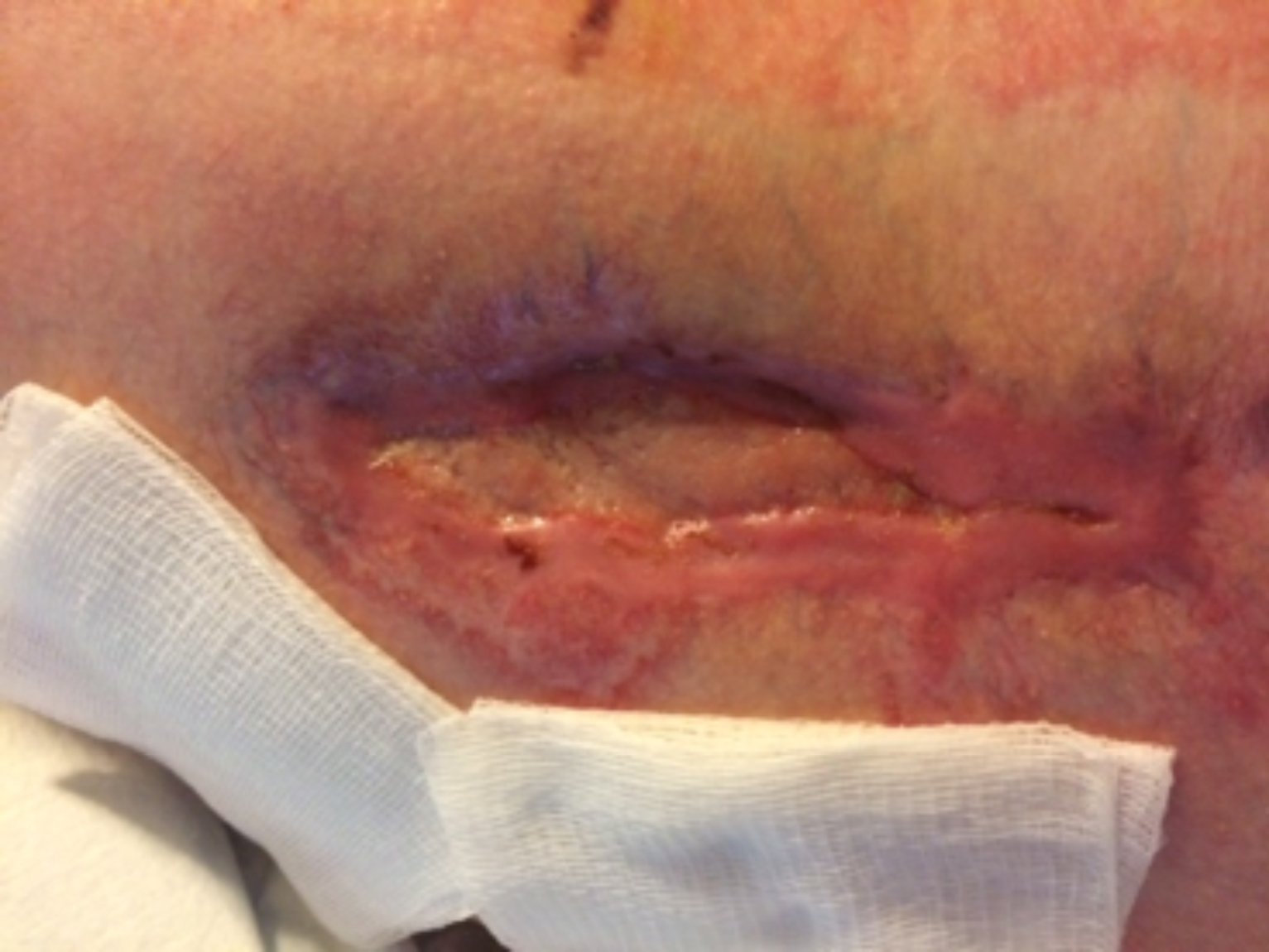 Figure 5. February 14th, 2016
Figure 5. February 14th, 2016
The role of surgery and when to do surgery is controversial due to the fear of the induction of pathergy. Although surgical procedures should be avoided in most cases when tissue necrosis presents a risk for infection or other more serious complications it still may have to be performed.
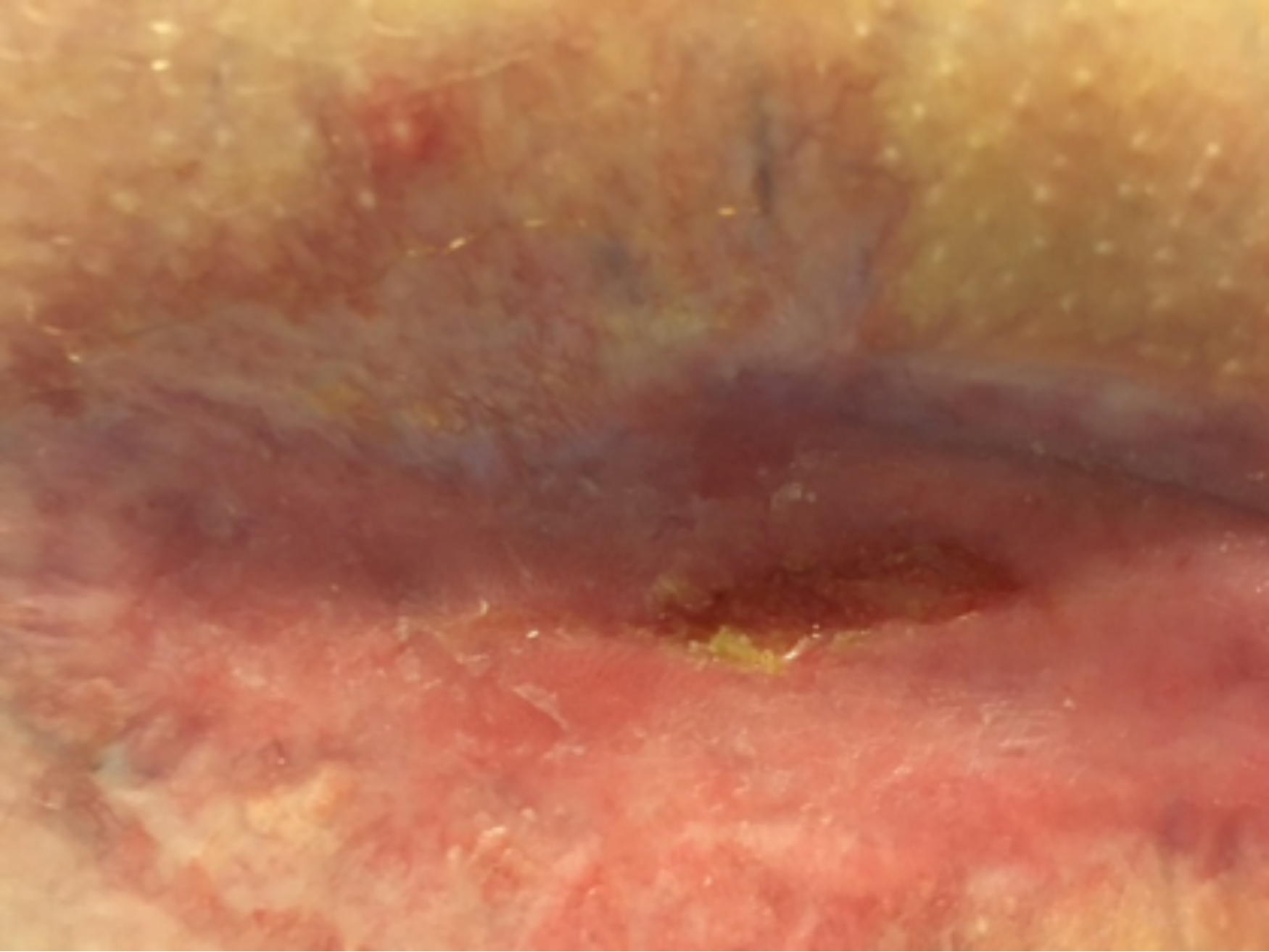 Figure 6. April 3rd, 2016
Figure 6. April 3rd, 2016
A retrospective review from the Mayo Clinic of 18 patients with PSPG was done for the purpose of stressing the importance of earlier recognition and prevention of improper/unnecessary surgery and the inherent complications. There were 18 patients with postoperative PG with an average age of 58 years; 15 (83%) were female. Sites of these patient’s wounds included seven breast, seven abdominal, one back, one shoulder, one ankle, and one scrotum, with breast reconstruction being the most common surgery. The average time to symptoms was 11 days. No patient had a fever, and five (27%) had leukocytosis. Because of these facts and an occasionally associated sterile culture, one should consider PG is the cause of the problem and not an infection. The conclusion was that although a rare surgical complication PG has a predilection for the breast and abdomen of females, and that early recognition may prevent unnecessary debridements and morbidity.
 Figure 7. May 30th, 2016
Figure 7. May 30th, 2016
Because a dilemma exists when and if debridement and/or skin grafting and/or future surgery is thought to be the best treatment for a patient but pathergy and the fear of causing a much larger wound is present, what are the options? One option is to delay the surgery until the wound is closed and another is to pretreat the patient with immunosuppressive drugs prior to surgery. Zachariah et al. has written about 3 cases in whom preoperative prestabilization of the ulcers with cyclosporine followed by successful split- thickness skin grafting was done. Kaddoura et al. and others have strongly recommended prophylactic steroids or immunomodulatory therapy.Zuo et al. discusses empiric therapy (oral prednisone 1mg/kg/d, methylprednisolone 0.5-1.mg/kg/d or Cyclosporine 5g/kg/d) for both prevention and treatment. Only when there is wound stabilization should corticosteroids be cautiously tapered.
When considering on how to prevent PSPG, awareness of the genetic association with PG is of extreme importance. Asking about the history of PG in the family is one of the most important questions that needs to be asked if not the most important, since the ability to easily obtain genetic studies currently is not available to the average clinician, but may be available in research institutions. PG is considered to be autosomal dominant. There are several syndromes that are currently identified that are thought to be due mutations located on chromosome 15q. There is the PAPA triad of pyogenic sterile arthritis, cystic acne and PG described in 1977 as well as PAPASH syndrome which includes pyogenic sterile arthritis, PG, acne and hidradenitis suppurativa. For these syndromes as well as for PG specifically, the hope is for better diagnostic tests as well as targeted and personalized therapies.
Prevention. Recognition. Treatment. If not recognized early the consequences can be serious. Taking a complete and thorough history from the patient’s and/or family is key. Treatment currently involves use of different types of medications with potential harmful side effects. The hope is to soon have a way to diagnose easily and treat with future targeted modalities. The knowledge that PG is hereditary/genetic is important now and for the future. This is most likely be the scientific discipline from where the answers will come.
References
1.Schadt C. Pyoderma Gangrenosum: Treatment and Prognosis. Up to Date. Ap 2016
2. Jackson J, James, Pyoderma Gangrenosum: Medscape Reference. April 26,2016
3. Tolkachjov SN, Fahy AS, Wetter DA, Brough KR, Bridges AG, Davis MD, Postoperative pyoderma Gangrenosum: The Mayo Clinic Experience of 20 years. J Am Acad Dermatol.2015 Oct; 73(4) 615-22
4. Tuffaha SH et al. Pyoderma Gangrenosum After Breast Surgery: Diagnostic pearls and Treatment Recommendations Based on a Systemic Literature Review Ann Plast Surg.2016 Aug;77(2)
5. Tolkachjov SN, Fahy AS, Cerci FB, Wetter DA,Cha SS, Camilleri MJ. A clinical review of published cases. J. Mayo Clin Proc.2016 Sep;91(9):1267-9
6. Zakhireh M, Rockwell B,Fryer R: Stabilization of Pyoderma Gangrenosum Ulcer with cyclosporine Prior to skin Grafting. Plastic and Reconstructive Surgery.2004;1417-1420
7. Kaddoura Il, Amm C. A Rationale For adjuvant Surgical Intervention In Pyoderma Gangrenosum.Ann Plast Surg 2001;46:23-8.
8. Zuo et al. Pyoderma Gangrenosum: identification of risk factors and proposed management strategy. British Association of Plastic, Reconstructive and Aesthetic Surgeons 2014; 68,295-303
9. Braswell S,et al. Pathophysiology of Pyoderma Gangrenosum: An updated review Am Acad Dermatol 2015;73: 691-8
