
Dr. Cadena is the current Chief of the Division of General Surgery at the Santa Fe Foundation in Bogota. He is currently the Executive Director of the Society of Surgical Infection for Latin America (SIS-LA) and is a part of the faculty of medicine of the Universidad de Los Andes as a Professor of General Surgery. He has also been a professor and instructor in the faculties of medicine of the National University de Colombia, the Javeriana University and the El Bosque University. Dr. Cadena has gained vast experience in his career as a general surgeon, especially in trauma and in the use of negative pressure for the management of abdominal compartment syndrome. Dr. Cadena has been a speaker in many conferences as well as national and international scientific congresses.
Cadena_Current Dialogues in Wound Management_2017_Volume 3_Issue 3
NOTE: As with any case study, the results and outcomes should not be interpreted as a guarantee or warranty of similar results. Individual results may vary depending on the patient’s circumstances and condition.
During the last two decades, there has been renewed interest in the concept of wound management of Necrotizing Fasciitis (NF), where local care is now included in a holistic view of the patient and not purely as a local phenomenon. This is a dynamic approach, in accordance with the pathophysiology and behavior of these wounds—that are usually rapidly lethal—and offers a conceptual basis for structured management, which makes it possible to achieve better results sooner.
The healing process is composed of a series of interrelated and interdependent events. These healing phases have been well established and their sequential occurrence – coagulation, inflammation, proliferation, and remodeling – makes it possible to obtain complete closure of the wound. However, any delay in one of these stages will lead to rapid deterioration, even to the point of death of the patient, as is the case with necrotizing fasciitis, where time is a crucial factor in the treatment of the patient.
The concept of wound bed preparation arose originally from the care of chronic wounds. Because it is a sequentially ordered treatment that encompasses both local and systemic aspects, it results in a powerful working tool when the wound puts the patient’s life at risk
The concept of wound bed preparation was introduced by Dr. Vincent Falanga and Dr. G Sibbald in 2000 based on the experience gained in the management of chronic wounds with special emphasis on the microenvironment of a wound, especially with regards to three factors: wound exudation, bacterial content, and devitalized tissue. In 2006, they extended this concept to the general context of the patient, involving patients’ general condition and comorbidities as first order conditioners in the healing process, i.e. a view of the complete patient, not one that is exclusively focused on the local aspect of the wound.
COMPONENTS
The acronym TIME groups the four components of this scheme that summarizes the handling of wounds in an orderly way.
T:Devitalized tissue (Tissue management)
I:Inflammation and infection (Inflammation and infection control)
M:Wound microenvironment (Moisture balance)
E:Epithelization (Epithelial edge advancement)
NECROTIZING INFECTIONS
Necrotizing soft tissue infections (NSTIs) rank among the more difficult disease processes encountered by physicians and surgeons. NSTIs can arise primarily in the dermis and epidermis, but they more commonly affect the deeper layers of adipose tissue, fascia, or muscle. NSTIs are typically caused by toxin-producing bacteria and are characterized clinically by very rapid progression of disease with significant local tissue destruction. Once symptomatic, the progression of disease is typically measured in hours; early diagnosis and treatment are crucial to survival. Diagnosis is hindered by the fact that the disease progresses below the surface, and the cutaneous manifestations belie the severity of disease. Even with optimal treatment,NSTIs portend significant morbidity and have mortality rates of 25%-35% in recent series
The management of this group of infections, recently grouped into three categories by Giuliano according to their etiological agent5, is widely favored, with the management scheme proposed by Falanga and Sibbald, because it is in this group of infections in which sequential management optimizes time—a critical factor to obtaining good results.
Devitalized tissue (tissue management)
The initial objective in these cases is the radical removal of all devitalized or infected tissue, carried out in the context of multidisciplinary management and preceded by an adequate treatment that makes it possible for the patient to be in the best possible condition to undergo the respective procedure, i.e. replenishment of circulating volume, wide-spectrum antibiotics, and required hemodynamic support.
The cornerstone in the treatment of necrotizing infections consists in complete debridement as soon as possible after diagnosis, as the delay in initial debridement is associated with an increase in mortality7,8. Resection of involved tissues should be conducted until healthy, bleeding tissue is found at all margins, this may require tissue resection beyond the delimited area of the skin as the process involves underlying tissues without necessarily being reflected at skin level. Sometimes even amputation may be required when a joint is involved. Necrotizing infections have the capacity to expand rapidly, even in the presence of adequate debridement, so re-examination should be planned within 24 hours.The average number of re-examinations are 3-4 per patient
Inflammation & Infection
Antibiotic coverage should be established from the beginning of treatment, concurrently with resuscitation, and empirical therapy should target Gram positive, Gram negative, and anaerobic germs. A useful scheme is penicillin G, which acts against Streptococcus and Clostridia; vancomycin which acts against Staphylococcus MRSA; clindamycin which, despite having a reduced spectrum, reduces the toxin production of clostridia and suppresses Tumor Necrosis Factor a, produced by monocytes and reduces M protein, a super-antigen produced by Streptococcus; a quinolone as treatment for Gram negative bacteria, because most of the time the renal function of these patients is affected, which limits the use of aminoglycosides. Therapy will continue until there is identification of the organism causing the infection, and only then will it be specifically targeted, once its sensitivity is known.
The wound microenvironment
The main objective in wound care is to obtain a healthy tissue, well vascularized and free of infection.
The use of negative pressure therapy, completely covering the wound, thus avoiding contamination, also decreases interstitial edema, which favors the revascularization of the affected tissue, thus improving the arrival of oxygen, nutrients, and antibiotics; on the other hand, it removes the toxic waste produced by the germs that cause the process from the wound bed, also allowing the continuous evaluation of the remaining tissue in view of the possibility of progression of the disease that may require additional resection.
 Figure 1: External appearance of a necrotizing fasciitis of the thigh at Day 0.
Figure 1: External appearance of a necrotizing fasciitis of the thigh at Day 0.
Once the changes caused by the systemic inflammatory response have disappeared and the appearance of the granulation tissue is adequate, definitive coverage of the defect should be planned either by means of the placement of partial thickness skin grafts or rotation flaps, depending on the magnitude of the defect.
 Figure 2: Vascular involvement caused by thrombosis produces the resulting ischemia.
Figure 2: Vascular involvement caused by thrombosis produces the resulting ischemia.
The use of negative pressure therapy is involved in each stage of wound management:
T:It removes, debris, and interstitial edema
I:Reduce bacterial count (not Staph aureus), reduce inflammatory cytokines, increase growth factors activity
M:It maintains the humid environment of the wound avoiding drying by exposure to the environment
E:Macrotension forces approximate the edges of the wound decreasing the exposed area.
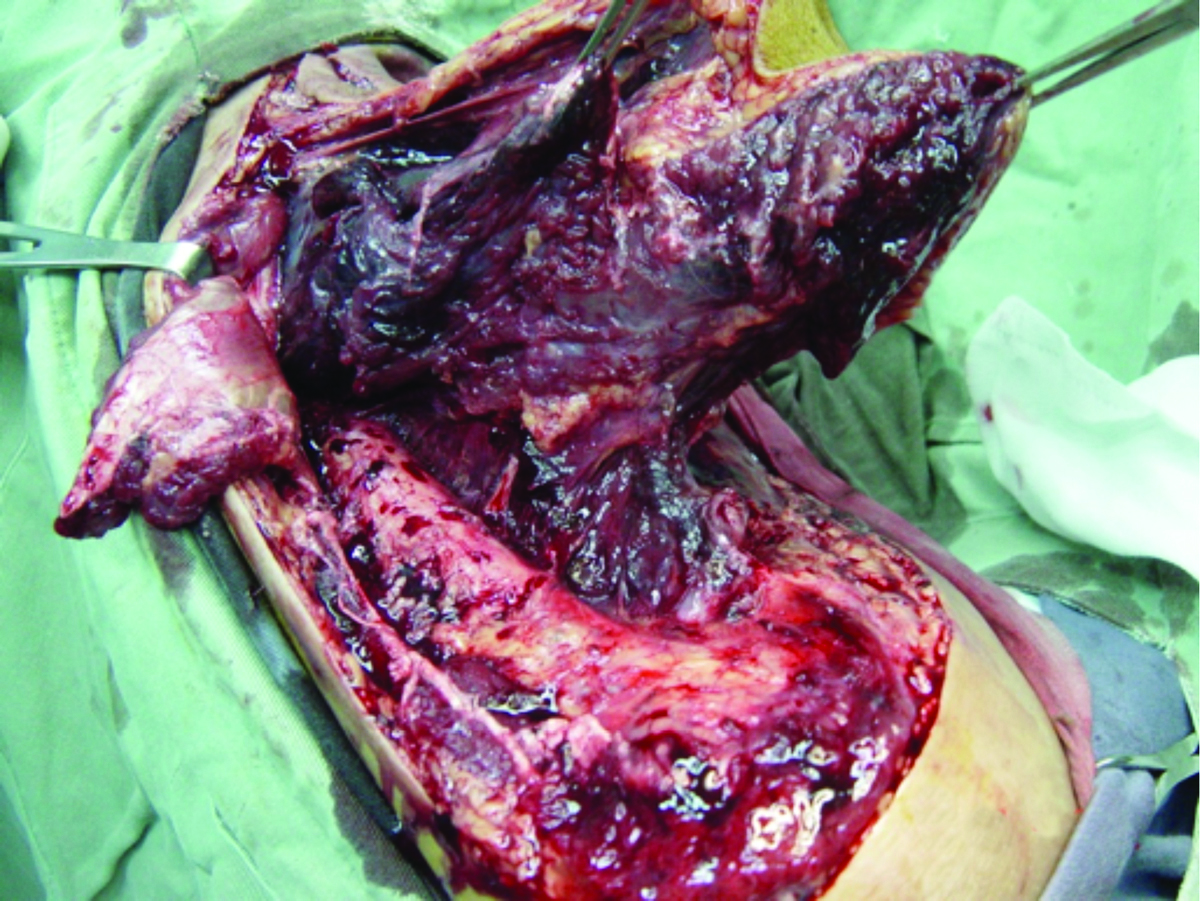 Figure 3: Appearance of myonecrosis.
Figure 3: Appearance of myonecrosis.
The concurrence of these phenomena causes a substantial shortening in the healing time of these wounds, which often require long periods of hospitalization and have a high risk of complication, in addition to high costs.Reduction of the wound area generated by the contraction of the borders, proliferation and migration of keratinocytes, are indicators of a wound healing properly; when these phenomena do not take place, it means there are one or more factors present that prevent healing.
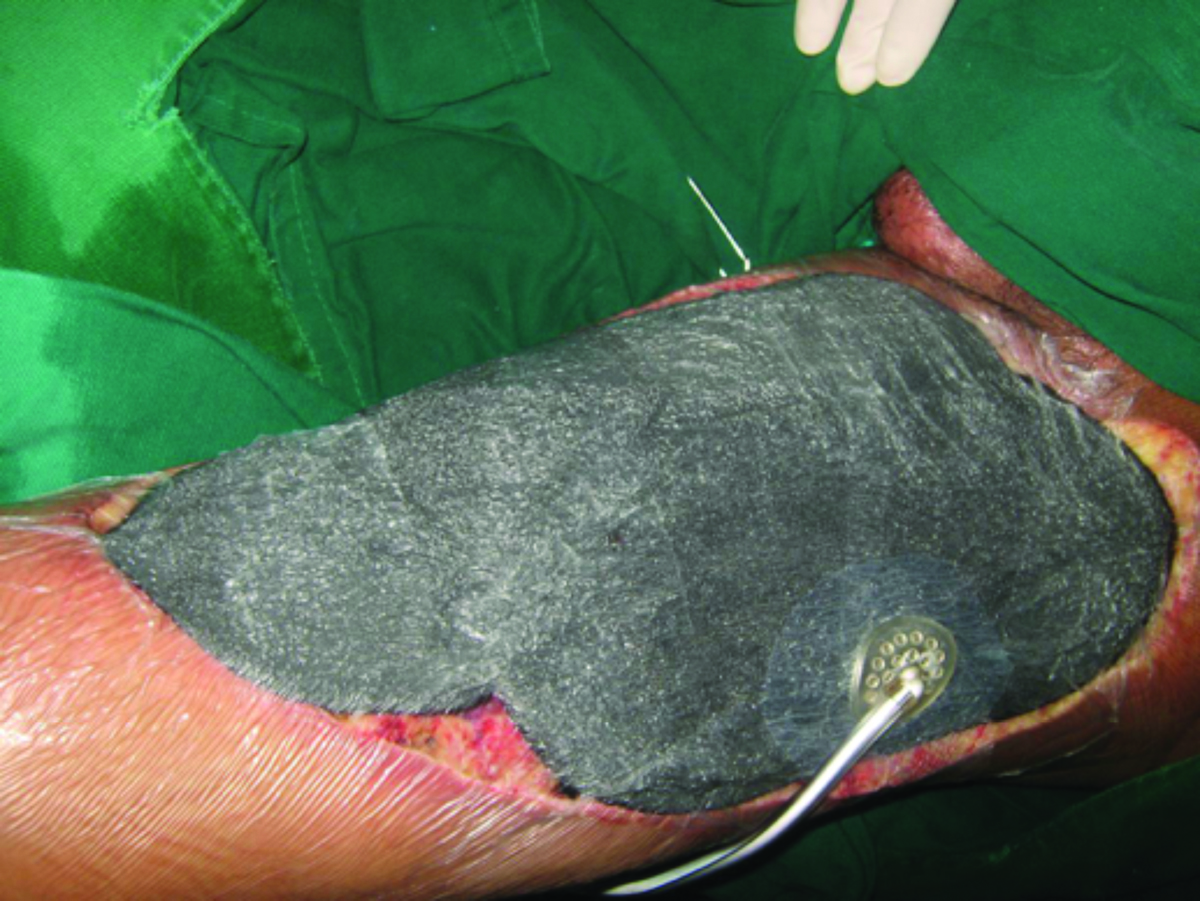 Figure 4: Negative pressure therapy affects each of the stages of wound healing.
Figure 4: Negative pressure therapy affects each of the stages of wound healing.
The use of negative pressure therapy in the management of necrotizing soft tissue infections offers the patient the ability to achieve favorable results in a shorter time, with a reduced hospital stay. It is imperative to obtain a debridement of the entire necrotic tissue early and to have a close surveillance of the wound, as the severity of these infections still has high mortality rates.Photos courtesy of Dr. Manuel Cadena Gutierrez and Dr. Diana Cadena
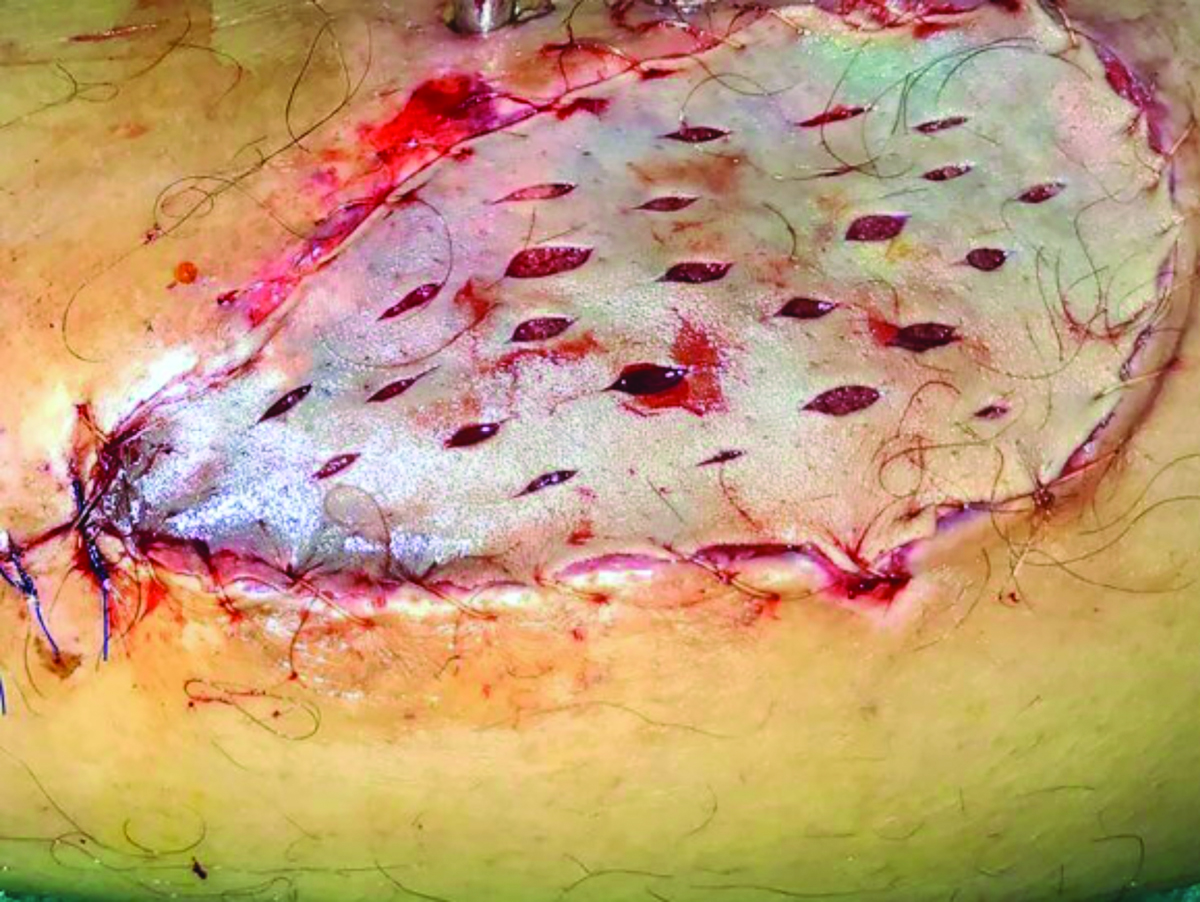 Figure 5: Final coverage will depend on the quality of the wound bed: Clean, free of infection, with adequate supply of oxygen and nutrients.
Figure 5: Final coverage will depend on the quality of the wound bed: Clean, free of infection, with adequate supply of oxygen and nutrients.
References
1.Schultz, Gregory S., et al. “Wound bed preparation and a brief history of TIME.” International wound journal 1.1 (2004): 19-32.
2.Cavanagh, Peter R., et al. “Treatment for diabetic foot ulcers.” The Lancet 366.9498 (2005): 1725-1735.
3.Schultz, Gregory S., et al. “Wound bed preparation and a brief history of TIME.” International wound journal 1.1 (2004): 19-32.
4.Hakkarainen, Timo W., et al. “Necrotizing soft tissue infections: review and current concepts in treatment, systems of care, and outcomes.” Current problems in surgery 51.8 (2014): 344.
5.Giuliano, Armand, et al. “Bacteriology of necrotizing fasciitis.” The American Journal of Surgery 134.1 (1977): 52-57.
6.Misiakos, Evangelos P., et al. “Current concepts in the management of necrotizing fasciitis.” Frontiers in surgery 1 (2014).
7.Freischlag, Julie A., George Ajalat, and Ronald W. Busuttill. “Treatment of necrotizing soft tissue infections: the need for a new approach.” The American journal of surgery 149.6 (1985): 751-755.
8.Goodell, Kristen H., et al. “Rapidly advancing necrotizing fasciitis caused by Photobacterium (Vibrio) damsela: a hyperaggressive variant.” Critical care medicine 32.1 (2004): 278-281.
9.Huang C, Leavitt T, Bayer LR, Orgill DP. Effect of negative pressure wound therapy on wound healing Curr Probl Surg. 2014 Jul;51(7):301-31.
