
Dr. Orgill is Vice Chairman for Quality Improvement in the Department of Surgery at Brigham and Women’s Hospital and Professor of Surgery at Harvard Medical School. He is a reconstructive plastic surgeon and has a PhD from MIT in Medical Engineering. He is the Director of the Brigham and Women’s Hospital Wound Care Center and runs a tissue engineering and wound healing Laboratory. His lab at BWH is working to develop better technologies to treat wounds including work with artificial skin, micromechanical forces, platelets and stem cells. He has consulted for several medical device and start-up companies and is the inventor on several patents. He worked on the team that developed Integra®, a skin replacement therapy that has been commercially developed and used successfully on thousands of patients.
Orgill_Current Dialogues in Wound Management_2017_Volume 3_Issue 3
NOTE: As with any case study, the results and outcomes should not be interpreted as a guarantee or warranty of similar results. Individual results may vary depending on the patient’s circumstances and condition.
INTRODUCTION
Advances in the treatment of chronic wounds have allowed many complicated wounds to heal using non-operative measures. One challenge in dealing with complex wounds is bacterial contamination particularly in the form of a biofilm. Biofilms are defined as microrganisms that stick to themselves and often are found on a self-produced polymeric substance. Biofilms are difficult to assess and many clinicians just assume that if a wound doesn’t heal it is due to biofilms. Because we don’t have a direct and easy clinical way to measure biofilms, several technologies that may address biofilms have been developed and marketed. These include antimicrobial solutions, ultrasound, shock wave, enzymatic debridement, and jet irrigation. We know that bacteria in wounds can often track deep around blood vessels and other structures making topical application of antimicrobial solutions unlikely to diffuse in sufficient quantity to kill all the bacteria. We do know that biofilms, even when disrupted, can re-form quickly possibly due to incomplete removal of bacteria. The purpose of this article is to discuss the well-known principle of excisional surgical debridement that may be the standard to which other modalities should be measured.
We see many patients in our clinic that have been on a wide variety of wound cleaning strategies and we can simply surgically close their wounds by excisional debridement followed by a flap or skin graft for closure. Certainly, if we could predict patients that will not heal with less invasive products and procedures, earlier surgical intervention would reduce the time wounds are open and avoid many complications that we see with chronic open wounds.
 Figure 1A: Chronic Stage 4 Sacral Pressure Injury
Figure 1A: Chronic Stage 4 Sacral Pressure Injury
WHAT IS COMPLETE EXCISIONAL DEBRIDEMENT?
Complete excisional debridement involves excision of the entire wound and taking a small amount of surrounding normal tissue. Typically, this would include the wound surface and about 0.3 to 0.5 cm of tissue around the wound. Very often this is done in preparation for a procedure where the wound can be closed such as a skin graft or a local flap. We often think of this in a similar fashion as an excision of a low grade malignancy, where the entire wound surface with a small margin needs to be removed.
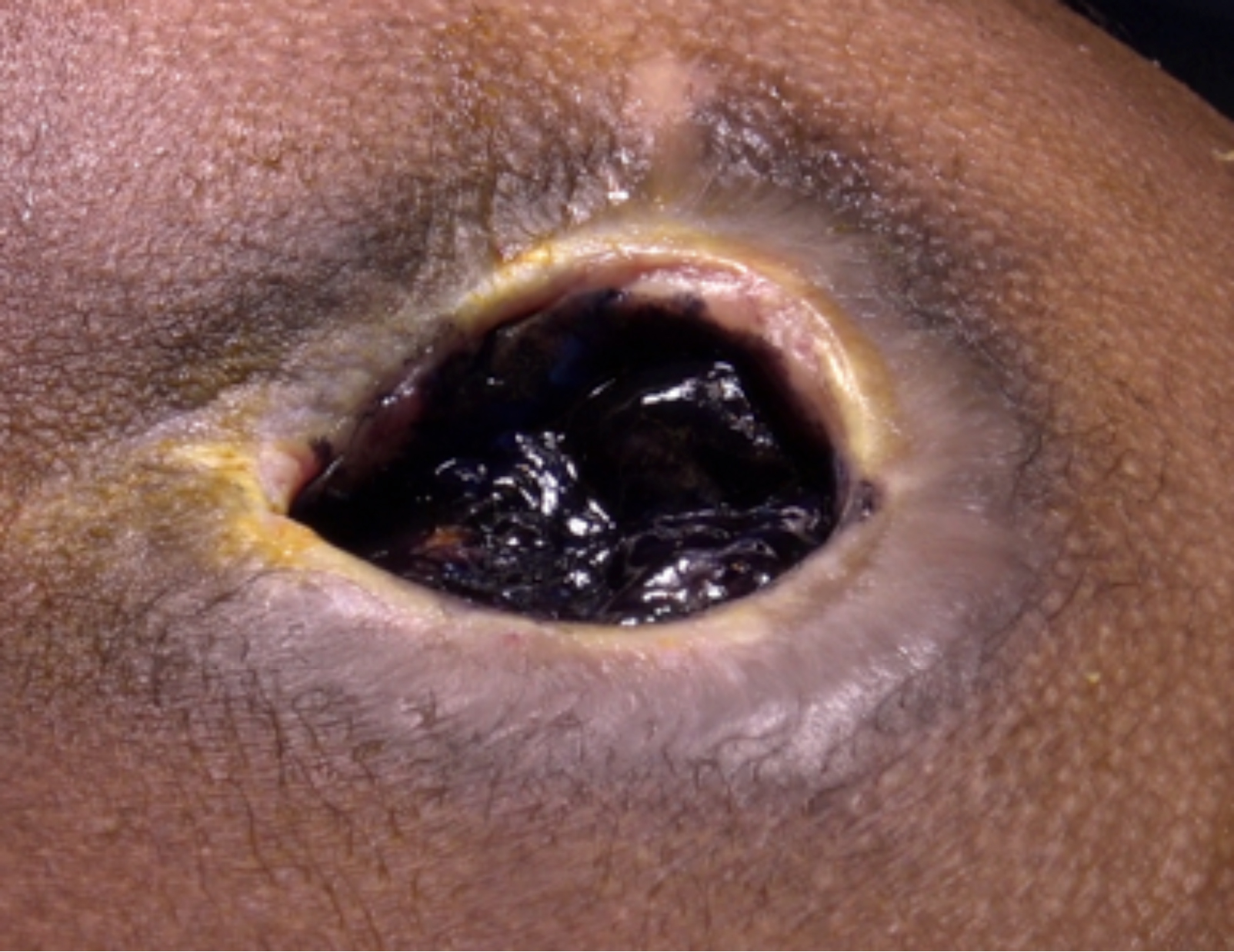 Figure 1B: The Injury is painted with methyelene blue
Figure 1B: The Injury is painted with methyelene blue
WHAT SPECIFIC TECHNIQUES ARE USED IN COMPLETE EXCISIONAL DEBRIDEMENT?
We like to infuse a dilute solution of local anesthesia and epinephrine (tumescent solution) around the wound in advance to minimize blood loss. We do this at the beginning of the case and allow about 15 minutes to pass. In most areas, the wound can be rapidly excised with a surgical scalpel. If the wound extends into the muscle, we like using a pinpoint electrocautery to remove the deep portions of the wound. For complex wounds that track, staining them with methylene blue can facilitate visualization and help ascertain that the entire wound has been excised. In many complex wounds, they are more easily excised taking the wound out in several pieces. Many wounds have bone at their base that can be excised with an osteotome. Deep bone cultures can be obtained after excision to determine if long term antibiotics are needed. All of these wounds are colonized with
 Figure 1C: After injection of lidocaine with epinephrine, the ulcer can be largely excised with the knife taking 4 to 5mm of normal tissue around it.
Figure 1C: After injection of lidocaine with epinephrine, the ulcer can be largely excised with the knife taking 4 to 5mm of normal tissue around it.
HOW DO I CLOSE THE WOUND AFTER COMPLETE EXCISIONAL DEBRIDEMENT?
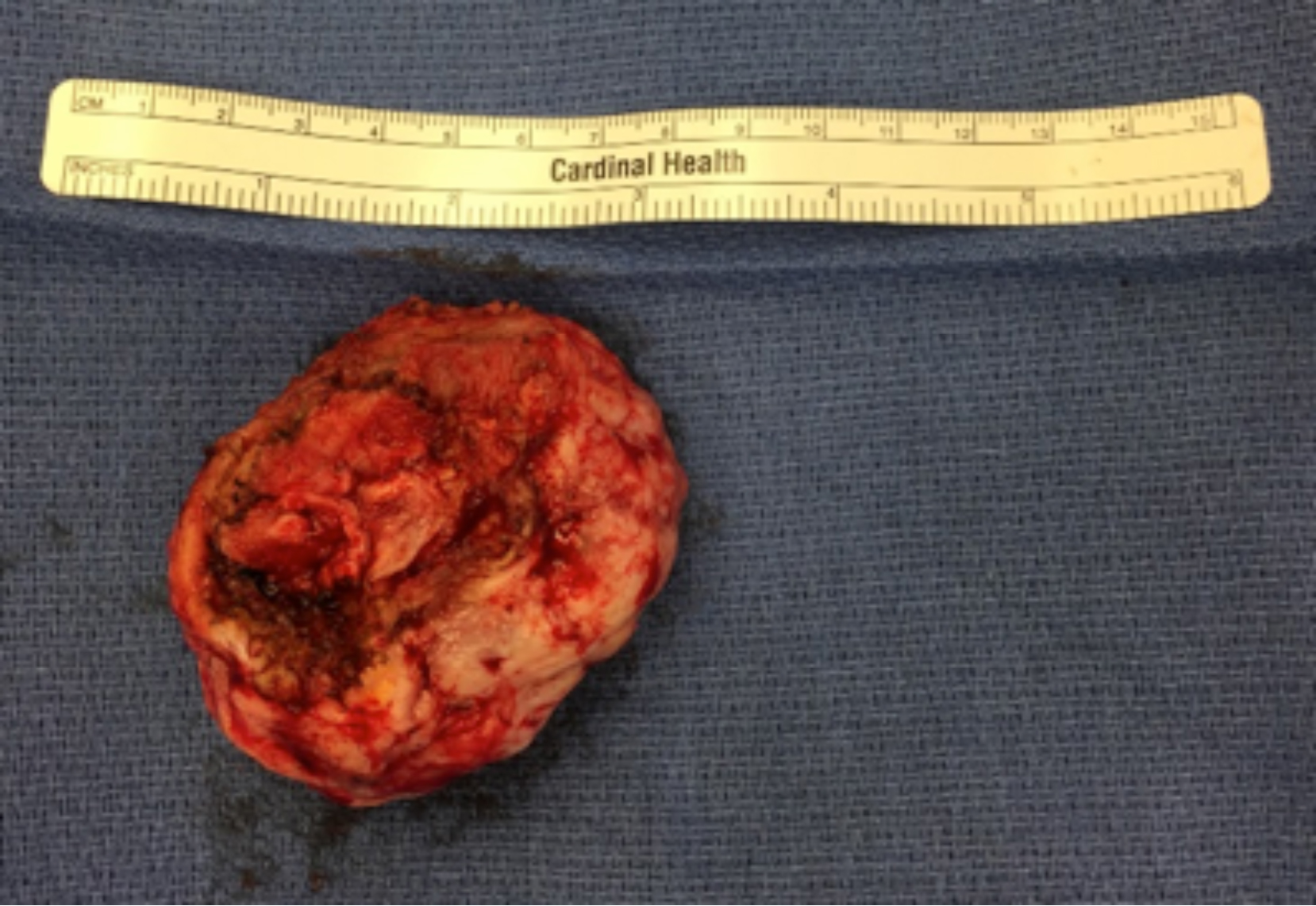 Figure 1D: A complete excision – note that no methylene blue is visible on the underside of the excision indicating that the entire ulcer surface has been excised.
Figure 1D: A complete excision – note that no methylene blue is visible on the underside of the excision indicating that the entire ulcer surface has been excised.
A variety of methods can be used for wound closure. For large areas, such as in a burn, split-thickness skin grafts harvested from an unburned area of the body can be grafted directly onto the excised area.1 For smaller areas that are deep, such as a pressure sore, local flap closure is quite effective.
WHEN DO I NOT CLOSE THE WOUND?
Patients that are recovering from sepsis and have a lot of purulence in the wound are at increased risk for septic events after debridement. In these cases, we will generally do a debridement of just the necrotic and infected tissues and not try to fully excise the wound. Often, we will use a Negative Pressure Wound Therapy (NPWT) device, with or without instillation to clean the wound up and facilitate shrinkage. Once the wound is smaller, complete excisional debridement can be performed.
 Figure 1E: After closure with a modified V to Y advancement flap.
Figure 1E: After closure with a modified V to Y advancement flap.
WHICH PATIENTS ARE NOT CANDIDATES?
Many patients with wounds have significant co-morbid disease states and are not good surgical candidates. Many wound patients have poor nutrition that should be optimized prior to closure. If there is a question about nutrition, we check albumin and pre-albumin levels and may delay excision and closure until nutritional status is optimized. Wounds need to be well drained and the patient should not be in a septic state prior to attempting closure. Patients that have mobility disorders and are unable to stay off their wounds in the post-operative period should have this procedure delayed until adequate positioning can occur.
Bleeding is always a concern. Many patients with complex wounds have had intense angiogenesis in their wound areas and can lose a moderate amount of blood during excision. Large perforating vessels can result in substantial bleeding over a short period of time. Many of our patients are anti-coagulated and may not be completely reversed prior to surgery. NPWT devices can rapidly remove blood from the wound and should be equipped with an alarm to indicated excess fluid removal. If this occurs, the device should be shut off and efforts directed towards hemostasis should be pursued.
SUMMARY
Complete excisional debridement is an efficient surgical method to excise the wound and prepare it for direct closure by a skin graft or flap. Doing this requires substantial surgical skill and judgment. It has the advantage of being a definitive and rapid method to prepare complex wounds for closure.
References
Orgill DP. Excision and skin grafting of thermal burns. New England Journal of Medicine. 2009 Feb 26;360(9):893-901.
