
Kersten Reider received her Diploma in nursing from the Reading Hospital School of Nursing and then went onto finish her BSN at Alvernia University. She is currently enrolled in the Adult-Geriatric Nurse Practitioner Program at Bloomsburg University. Kersten is a Certified Wound, Ostomy, Continence nurse (CWOCN) who serves as an in-patient wound, ostomy, and continence specialist for a licensed 700 + bed Level II Trauma Center in West Reading Pennsylvania. She focuses on the care of surgical patients with an interest in nursing and physician education along with fistula management and negative pressure wound therapy. Kersten has presented posters as well as spoken nationally regarding fistula management and wound care. She has also published articles on fistula related topics.
Reider_Current Dialogues in Wound Management_2017_Volume 3_Issue 3
NOTE: As with any case study, the results and outcomes should not be interpreted as a guarantee or warranty of similar results. Individual results may vary depending on the patient’s circumstances and condition.
ABSTRACT
BACKGROUND: Seventy-year-old female with an extensive medical and surgical history related to Crohn’s disease admitted with an obstructing chronic terminal ileum unresponsive to maximum medical therapy. The patient underwent surgical intervention, which resulted in an anastomotic leak and incisional dehiscence. Re-exploration led to the creation of an ileostomy in close proximity to a large midline abdominal wound. The ileostomy became ischemic, retracted into a skin fold, and leaked enteric content through a tunnel under intact skin into the midline abdominal wound.
METHODS: Negative pressure wound therapy (NPWT) was utilized to granulate and contract the abdominal wound while ostomy appliances, along with accessory products, were used to contain effluent. The ostomy appliances leaked several times a day, due to location and structure, causing severe peristomal skin breakdown. Fistula isolation devices were used as a wall between the stoma and the abdominal wound to prevent effluent from entering the wound bed as well as direct it away from the peristomal skin while utilizing NPWT at -125mmHg. Dressings were changed three times per week.
CONCLUSION: The use of fistula isolation devices, in conjunction with NPWT and an appropriate ostomy appliance, produced positive patient outcomes (such as patient-reported satisfaction, promotion of wound healing, resolution of peristomal skin damage, reduced use of pain medication, and discharge to home with visiting nurses) in this patient.
INTRODUCTION
Not all wounds are cookie cutter wounds. Not all ostomies are constructed perfectly. When these become difficult to manage due to uncontrollable circumstances they become a wound, ostomy, and continence nurse’s challenge. A hostile abdomen does not need to cause a patient distress. With the use of specialty products and creativity, positive patient outcomes can be achieved.
CASE
A seventy-year-old female with an extensive medical and surgical history related to her Crohn’s disease presented to the Emergency Department with diffuse abdominal pain, distention, nausea, and no bowel movement for three days. During the admission interview, she reported that her symptoms had been persistent for a few days and present similarly to when she developed a bowel obstruction in the past. CT scan of abdomen and pelvis revealed multiple dilated loops of small bowel within the right lower quadrant and mid abdomen concerning for a high-grade partial or early small bowel obstruction. Based on the clinical history and exam, labs or imaging studies there was no indication for acute operative intervention. At this time, the decision was made to admit the patient to medical-surgical unit for conservative management which included not allowing the patient to eat, IV fluids, pain control, and a nasogastric tube (NGT) if vomiting. Due to the patient’s history of Crohn’s disease, a consult to a gastrointestinal specialist was requested for medical management. Over the course of a week, the patient’s symptoms decreased in severity but she still complained of pain after eating. Her persistent complaint of abdominal pain led the surgeon to order a small bowel follow through. The results indicate a very tight stricture of the terminal ileum without evidence of abscess along with two small fistulous tracts between small bowel to small bowel and small bowel to cecum.
Unfortunately, the patient’s high-grade partial obstruction failed maximum medical therapy and surgical intervention became necessary. The patient underwent an exploratory laparotomy, extensive adhesiolysis, ileocolic resection with primary anastomosis. During the surgical procedure, the patient was found to have a dense phlegmonous adhesive mass in the right lower quadrant at the location of her obstruction. This required extensive adhesiolysis for mobilization and ultimate resection. When the resection had been completed back to palpably normal bowel, a primary ileocolic anastomosis to the level of the distal ascending colon was completed and the midline incision was closed. Post operatively an NGT was placed until return of bowel function, two units of packed red blood cells were transfused for a hemoglobin of 7.0 and a hematocrit of 22.9, and patient controlled analgesic (PCA) pump was started for pain control. Over the next few days following surgery, the patient’s white blood cell count slowly increases, her abdomen becomes mildly distended, there is erythema along the abdominal incision line, she is tachycardic and shows signs of confusion.
Three days post-operatively a medical assessment treatment team (MATT) is called due to the patients change in mental status with agitation. During the assessment, the patient complains of increasing abdominal pain and distention is noted. At this time the patient was transferred to the intensive care unit for closer monitoring. Bleeding from the abdominal incision is noted by the bedside nurse over a two-day period. On the third day, incisional dehiscence with fascial separation and small bowel evisceration is reported and operative intervention is necessary. Intra-operatively it was found that the suture had pulled through the tissues because there was no breakage of the suture. She was found to have a few small collections of clotted blood that were evacuated. Additionally, during mobilization of the bowel to confirm the absence of a large right sided hematoma, there was found to be a small amount of enteric content in the right upper quadrant. On further exploration, there was found to be a small defect on the colonic side of the staple line of the anastomosis but no actual contamination of the abdominal cavity. Necrosis of staple line did not allow for restoration of the continuity therefore the ileocolic anastomosis was resected and an ileostomy created in the right upper quadrant. Retention sutures were placed at the level of the ostomy and then the fascia was closed from above and below taking care to avoid underlying structures. The surgeon then applied betadine dampened kling (DeRoyal Industries Inc. Powell, TN) into the abdominal wound and covered with a bulky dry dressing. The patient was then transferred to the intensive care unit. Over the next several days, the patient is requiring ventilator support for post-operative respiratory failure, her white blood cell count continues to rise, she is tachycardic, hypertensive, her NGT outputs are high, and the wound, ostomy, continence nurse (WOCN) is consulted for ostomy education.
 Figure 1: Necrotic stoma with tunneling under intact skin into abdominal wound. 18 x 10.5 x 3.3cm
Figure 1: Necrotic stoma with tunneling under intact skin into abdominal wound. 18 x 10.5 x 3.3cm
assessed by the WOCN. It was noted that her abdominal wound was packed with betadine soaked gauze and her stoma showed signs of ischemia. On post op day six the surgeon requested the wound be treated with NPWT. Upon assessment of the abdominal wound, there were retentions sutures in place, the wound base was red, concerns for fascial breakdown, and increase serosanguinous drainage noted. The ostomy appliance contained dark, liquid effluent. At this time, NPWT was applied to the wound utilizing white foam to the wound base followed by black foam with negative pressure at 75mmHg to promote granulation tissue. A two piece stretch to fit wafer with drainable bag was applied to the ostomy. This treatment plan was continued for approximately four days until feculent drainage was noted in the JP drain in the patient’s right lower quadrant. Was this a questionable enterocutaneous fistula from a previous placed JP drain? The decision was made to discontinue NPWT and pack the abdominal wound with Dakin’s infused gauze packings until further assessment could be accomplished.
Over the course of ten days, the wound continues to be packed with Dakin’s infused gauze, the stoma continues to deteriorate causing the ostomy appliances to leak frequently, and a connection between the ostomy and wound is noted. Assessment by the WOCN revealed a necrotic stoma that retracted into a skin fold with a circumferential mucocutaneous separation. Upon further assessment, it was noted that the effluent from the stoma was tracking under intact skin and pooling in the base of the abdominal wound (Figure 1). The wound measured 18 X 10.5 x 3.3 with a 4cm tunnel at 9:00, at this time the decision was made by the WOCN to try to wall off the connection between the stoma and abdominal wound to prevent effluent from entering the wound while promoting granulation tissue and wound contraction.
 Figure 2: Application of Fistula ISOLATOR STRIP® and NPWT
Figure 2: Application of Fistula ISOLATOR STRIP® and NPWT
A fistula ISOLATOR STRIP® was cut and fit along the right lateral wound wall to keep the effluent from the stoma from entering the wound bed. NPWT was then placed utilizing white foam to the friable wound base and then filled with black foam at -100mmHg. (Figure 2). A convex ostomy appliance was placed over the stoma to contain effluent and a fecal containment device was placed over the old JP drain site to collect the feculent drainage. This particular treatment plan was continued for a few days until the patient returned to the operating room for drainage of an abdominal abscess that extended from the site of the old JP site into the right Iliac crest. While in the operating room, the surgeon had considered revising the patient’s stoma that had retracted 2cm below skin level but unfortunately mobilization was not achieved. Now with a new surgically created wound in the right lower abdomen the WOCN decided to utilize NPWT to this area bridging to the midline abdominal wound. Over the next month the treatment plan consisted of utilizing a fistula ISOLATOR STRIP® to the right lateral wound wall to keep stoma effluent from entering the wound bed. At this point there was no concern for fistula development in the midline wound, and NPWT was applied to the wound base utilizing black foam with negative pressure at -100mmHg. During this period, there was production of granulation in the wound bed, the tunnel from the stoma to the wound had closed, and the wound edges had contracted significantly. All these positive patient outcomes led to the discontinuation of NPWT and application of a local wound dressing that could be managed by the patient or visiting nurses (Figure 3).
 Figure 3: Progression of the wound utilizing a fistula ISOLATOR STRIP® and NPWT
Figure 3: Progression of the wound utilizing a fistula ISOLATOR STRIP® and NPWT
Despite the patient’s positive outcomes with her abdominal wound, there still remained the issue of a high output ileostomy and a continually leaking ostomy appliance. Several different ostomy appliances and accessory products had been utilized in the attempt to contain the effluent with no success. On average the ostomy appliances needed to be changed two to three times a day. Frequent leaking of the ostomy appliance caused the patient’s peristomal skin to become severely denuded requiring intravenous pain medication for appliance changes (Figure 4). Leaking of the ostomy appliance became a barrier to the patient’s discharge. The patient could not independently care for her ostomy appliance at home, rehab facilities had refused her admittance due to a complicated ostomy, visiting nurse associations felt she needed a higher level of care, and she did not meet the requirements for a skilled nursing facility. The WOCN was tasked with creating an appliance that would have an increase wear time, allow the patient to be more independent, and ultimately return home with visiting nurses. Assessment of the stoma revealed a
 Figure 4: Denuded peristomal skin from leaking ostomy appliance and high output stoma
Figure 4: Denuded peristomal skin from leaking ostomy appliance and high output stoma
contracted stoma located in a skin fold with a circumferential mucocutaneous separation that was functioning for high output. Since the stoma resided in a skin fold, there needed to be some kind of conduit for the effluent to flow through and be directed into the ostomy appliance. A WOUND CROWN® was utilized as a conduit that was cut to fit around the stoma and fit snuggly into the skin fold. The WOUND CROWN® was fit into a two-piece cut to fit ostomy appliance with a belt to ensure security (Figure 5). The use of the WOUND CROWN® proved to be successful. The ostomy appliance remained in place for two days with
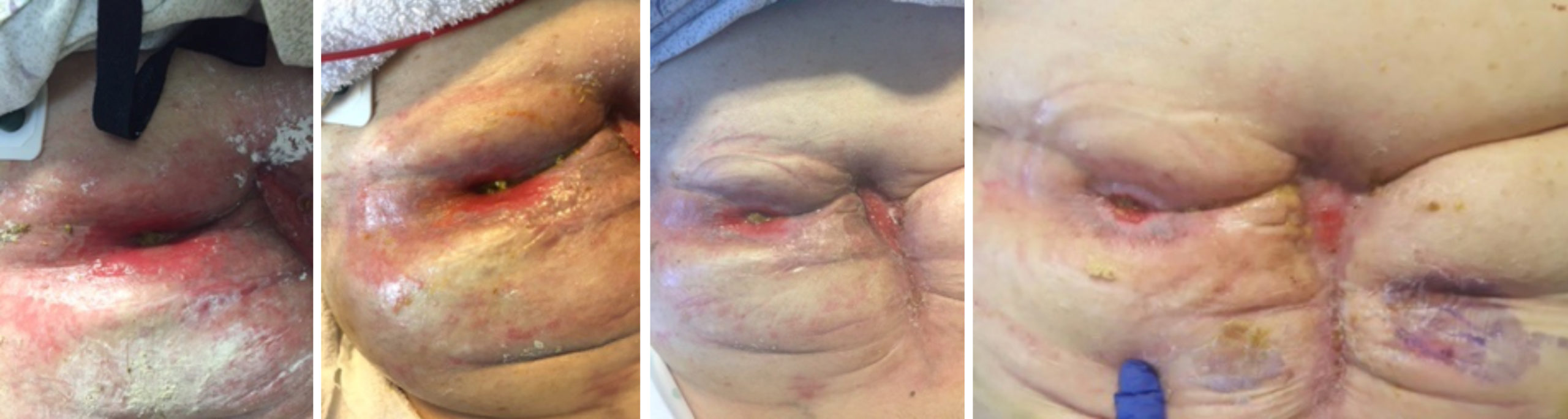 Figure 6: Progression of peristomal skin with the use of WOUND CROWN® and ostomy appliance
Figure 6: Progression of peristomal skin with the use of WOUND CROWN® and ostomy appliance
no leaking. Her peristomal skin significantly improved within two weeks which resulted in the reduction in pain medication consumption (Figure 6). Due to the complexity of the ostomy appliance application, vising nurses along with the patient and family members were provided detailed bedside and written instructions so that the patient could return home upon discharge. Three months after initial presentation, the patient’s hostile abdomen had become manageable. Her abdominal wound had contracted significantly measuring 2 x 1 x 0.3cm and required only a local wound dressing change every two days. The patient continued to utilize the WOUND CROWN® with an ostomy appliance which resolved her peristomal denuded skin and remained in place for two days. In this particular case the use of fistula isolation devices for both the wound and ostomy along with NPWT proved to be a beneficial necessity for this patient.
 Figure 5: The utilization of the WOUND CROWN® as part of the ostomy appliance
Figure 5: The utilization of the WOUND CROWN® as part of the ostomy appliance
NOTE: The WOUND CROWN®, FISTULA FUNNEL®, and ISOLATOR STRIP® are manufactured by FISTULA SOLUTION®. KCI is the exclusive distributor. Please consult a clinician and product instructions for use prior to application.
References
