
Dr. Dardano is a board certified plastic and reconstructive surgeon in Boca Raton, Florida. He earned his medical degree from Nova Southeastern University. He completed his general surgery residency at Wayne State University in Detroit, and his plastic surgery fellowship at the University of Texas Medical Branch in Galveston. He has completed specialty training in Burn surgery, Microsurgery, and Cosmetic surgery. He is double board certified by the American Board of Surgery, and The American Board of Plastic Surgery. He is an active member of the American Society of Plastic Surgeons, and the American Society of Aesthetic Plastic Surgeons. He is a Fellow of the American College of Surgeons and is the Vice President of the International College of Surgeons. he has written text-book chapters, and has lectured internationally on various subjects within plastic surgery. He currently serves as Chief of Staff at Boca Raton Regional Hospital. In addition to his clinical practice, he is an Associate Professor of Biomedical Sciences and Surgery at FAU College of Medicine as well as the program director of the general surgery residency program.
Dardano, Quiresi and Klapper_The Chronicles of Incision Management_2017_Volume 1_Issue 2
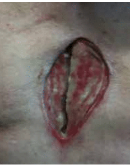
We present the case of a 72-year-old male with atrial fibrillation, prior tobacco use, coronary artery bypass graft (CABG), and an aortic valve repair at another hospital. He underwent several attempts at surgical debridement and pectoralis muscle flap closure of dehisced sternal wound by a cardiothoracic surgeon (see Figure 1).
His cultures remained positive for MRSA (methicillin resistant staph aureus) following the repair, and his wound dehisced again. He was discharged to a cardiac rehabilitation facility and nursing home with an open sternal wound.
His wound care consisted of wet-to-dry normal saline dressings. He was referred to the plastic surgery service for evaluation at which point the patient was admitted to the hospital and started on empiric IV vancomycin and cefepime. His cultures on admission were positive for MRSA and vancomycin-resistant enterococcus (VRE). He was taken to the operating room for surgical debridement of the sternum with washout of the wound and placement of V.A.C. ULTA™ Therapy System to be certain that the mediastinum and chest cavity was sealed.
He was taken back to the operating room on post-operative day 4 for placement of V.A.C. VERAFLO™ Dressing. It was safe to place the V.A.C. VERAFLO™ Dressing on the mediastinum since the mediastinum had developed a base of granulation with no communication with the pleural cavity. V.A.C. VERAFLO™ Therapy was initiated with normal saline with a soak time of 1 min and 1 hour of negative pressure wound therapy (NPWT 125 mmHg).

This was continued for 8 days until the wound cultures became negative. The patient was taken back to the OR for sternal reconstruction to stabilize the remaining bony sternum and ribs utilizing sternal reconstruction plates (DePuy Synthes). A rectus abdominis muscle flap was used to cover the plates and provide vascular coverage to the repair. The patient completed his course of antibiotics and his wound had completely healed. He was discharged home on clindamycin daily for life as prophylaxis.
NOTE: Specific indications, contraindications, warnings, precautions and safety information exist for KCI products and therapies. Please consult a clinician and product instructions for use prior to application. Rx only.
References
