
Emily Greenstein is a Certified Adult-Geriatric Nurse Practitioner and Certified Wound and Ostomy Nurse. She obtained her BSN for Jamestown University and MSN for Maryville University. She currently is employed by Essentia Health in Fargo, ND. She is the President for the North Central Region Wound, Ostomy, Continence Nursing Society. Emily is also on the Board of Directors for the American College of Clinical Wound Specialists. Ms. Greenstein is a paid consultant for Solventum.
Greenstein_Current-Dialogues-in-Wound-Management_2025_Article-6
Periwound skin management is a critical component of successful wound care focused on protecting and maintaining skin within a 4 cm area beyond the wound edge.1 Periwound is highly susceptible to damage from:
- Excessive exudate: Unmanaged wound fluid can lead to maceration, where the skin becomes “waterlogged” and vulnerable to further breakdown (Figure 1A).
- Adhesive trauma: Frequent dressing changes can lead to Medical Adhesive-Related Skin Injury (MARSI), including skin stripping or blistering (Figure 1B).
- Inflammation and infection: Exposure to bacteria or allergens in wound products can cause localized dermatitis (Figure 1C) or more severe complications, such as cellulitis (Figure 1D).
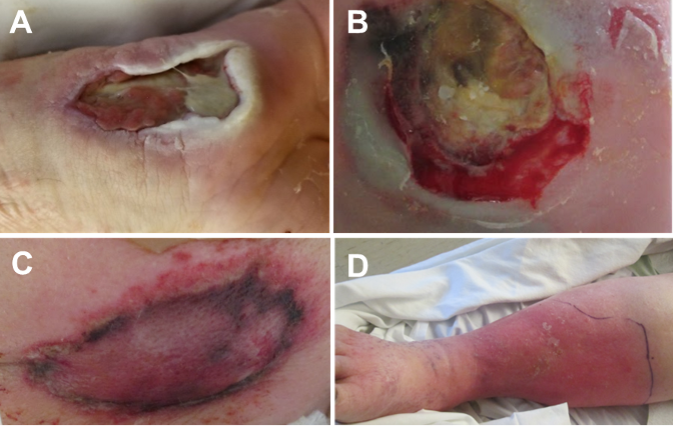
B. Adhesive trauma, in which frequent dressing changes have resulted in Medical
Adhesive-Related Skin Injury; C. Localized dermatitis caused by exposure to
bacteria or allergens in wound products; D. Cellulitis, a severe complication
resulting from exposure to bacteria or allergens in wound products. Images
courtesy of Emily Greenstein, APRN, CNP, CWON-AP, FACCWS
Effective periwound skin management requires a proactive approach centered on regular clinical assessment, rigorous moisture control, and the use of protective barriers to maintain a healthy periwound environment for healing. Additionally, skin can be more vulnerable in patients with certain comorbidities and conditions.
Periwound damage can contribute to delayed healing, worsened wound deterioration, increased wound size and infection risk, heightened pain and discomfort, reduced quality of life, and extended treatment duration and associated costs.2
PERIWOUND SKIN ASSESSMENT
Characteristics of the periwound and adjacent tissues can provide clues about the patient’s skin health, the phase of wound healing, and overall health status.1 Periwound skin should be assessed at every dressing change, focusing on:
- Color and temperature: Erythema or warmth may indicate an infection or inflammation; pale or cool skin may indicate vascular issues; and white or grey, softened skin may indicate maceration.
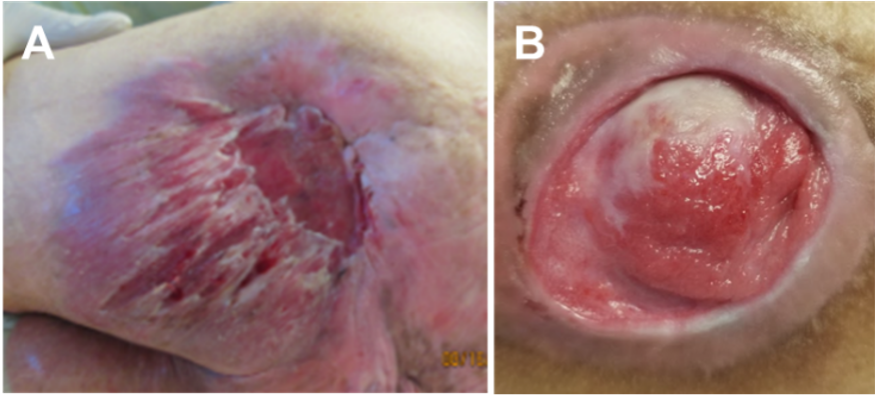
- Wound location: Note if the wound overlies a bony prominence, an area exposed to high friction/shearing forces (Figure 2A), or to incontinence, and document where periwound skin breakdown is occurring.
- Wound edges: Look for epibole (rolled edges, Figure 2B) or undermining, which can suggest chronic friction/shearing.
- Skin integrity: Check for thin, fragile skin that is more prone to tearing; assess the skin’s hydration for cracks, flaking, or maceration; and observe skin abnormalities such as calluses, edema, altered sensation, or scar tissue.
EXUDATE
Exudate, or fluid leaked from vessels, is important for wound healing. It provides a moist wound environment, enables the diffusion of immune mediators and growth factors, and promotes the separation of dead or damaged tissue through autolysis.3However, in chronic or hard-to-heal wounds, exudate contains high concentrations of proteolytic enzymes that can degrade the skin’s barrier, complicates management, and causes distress to the patient.4
High exudate levels may be indicative of underlying disease processes such as wound inflammation or infection.3,4Diagnosing infection or any other underlying disease process relies on a full assessment and investigation, as increased exudate production alone is insufficient evidence for diagnosis. Other factors that can contribute to high exudate production include prolonged periods with the wound in a gravity-dependent position, reduced willingness to cooperate with compression therapy, and development or worsening of congestive heart failure or peripheral edema. Conversely, low exudate production may occur in ischemic ulcers or reflect systemic problems such as dehydration.3,4
PERIWOUND SKIN PROTECTION
Managing periwound skin can be challenging as the fragile skin can be irritated by heavy exudate, or damaged by the application and removal of barrier creams and paste, which can also obscure the periwound area.5,6 However, 3M™ Cavilon™ Advanced Skin Protectant provides transparent periwound skin protection that allows for easier monitoring of the underlying skin and an easier application that can attach to wet, weepy, and damaged skin compared to other barrier creams and pastes. Cavilon Advanced Skin Protectant uses a polymer-cyanoacrylate technology to protect at-risk skin for up to 7 days and helps manage moderate to severe skin damage.
CASE STUDIES
Case 1
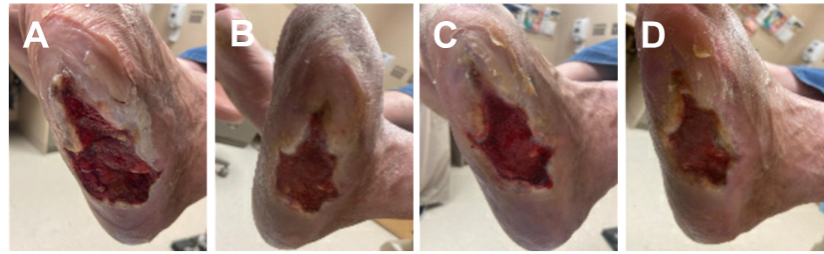
A 59-year-old male with a history of diabetes and reoccurring diabetic foot ulcer presented for care (Figure 3A). Following the patient and wound assessment, surgical debridement was performed followed by wound management using Solventum™ V.A.C.® Therapy using continuous negative pressure at -125 mmHg and dressing changes every 2-3 days. After 14 days, V.A.C.® Therapy was discontinued for use of silver hydrofiber dressings and a total contact cast. At the dressing change 7 days later, the periwound skin had developed maceration (Figure 3B). Cavilon Advanced Skin Protectant was applied to the periwound skin followed by dressing application and another total contact cast. When the cast and dressings were removed 7 days later, improved periwound skin condition was noted (Figure 3C). Continued periwound skin improvement was observed at the next dressing change 7 days later (Figure 3D).
Case 2
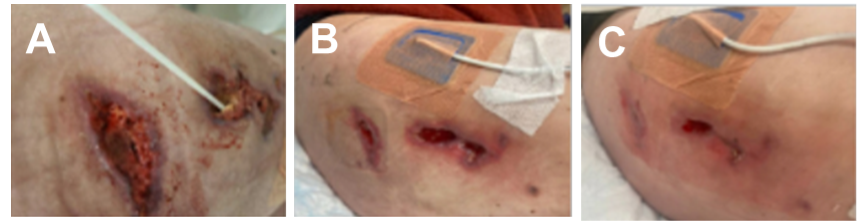
A 42-year-old female sustained a degloving injury to the right thigh following a motorcycle accident (Figure 4A). The patient underwent surgical debridement of the wound. Following use of wound care dressings, periwound skin irritation and breakdown was observed. Cavilon Advanced Skin Protectant was applied to the periwound skin followed by application of a collagen dressing, silver hydrofiber dressing, and foam border dressing (Figure 4B). Dressings were changed every other day and Cavilon Advanced Skin Protectant was applied once every 7 days. After 14 days of Cavilon Advanced Skin Protectant use, notable improvements in the periwound skin condition were observed (Figure 4C).
CONCLUSIONS
Periwound skin protection is a fundamental component of comprehensive wound management. The use of Cavilon Advanced Skin Protectant, offers a therapeutic advantage to help address the dual challenges of moisture management and maintaining clinical visibility, enabling continuous skin monitoring without the need to remove thick barrier pastes.
References
- Sussman C. Assessment of the skin and wound. In: Sussman C, Bates-Jensen B, editors. Wound care: A collaborative practice manual for health professionals. 4th ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins, 2012. P. 85-122.
- LeBlanc K, Beekman D, Campbell K et al. Best practice recommendations for prevention and management of periwound skin complications. Wounds Int. 2021. Available from:https://woundsinternational.com/best-practice-statements/best-practice-recommendations-prevention-and-management-periwound-skin-complications/
- Expert working group; Satellite expert working group. Wound exudate and the role of dressings. A consensus document. Int Wound J. 2008;5 Suppl 1(Suppl 1):iii-12. doi:10.1111/j.1742-481X.2008.00439.x
- Bianchi J. The effective management of exudate in chronic wounds. Wound Int. 2012; 3(4): 14-16. https://woundsinternational.com/journal-articles/the-effective-management-of-exudate-in-chronic-wounds/
- Greenstein E. Use of advanced elastomeric skin protectant on venous leg ulcer periwound skin. Wounds. 2023;35(2):E78-E81. doi:10.25270/wnds.22026.
- Hollinworth H. Challenges in protecting peri-wound skin. Nurs Stand. 2009;24(7):53-58. doi:10.7748/ns2009.10.24.7.53.c7330
NOTE: Specific indications, contraindications, warnings, precautions and safety information exist for these products and therapies. Please consult a clinician and product instructions for use prior to application. Rx only.
As with any case study, the results should not be interpreted as a guarantee or warranty of similar results. Individual results may vary depending on the patient’s circumstances and condition.
©Solventum 2026. Solventum, and S logo are trademarks of Solventum or its affiliates. 3M and the 3M logo are trademarks of 3M. All other trademarks are owned by their respective owners.
