
As a Double Board-Certified reconstructive and cosmetic Plastic Surgeon Dr. Saeed A. Chowdhry is a lifelong Chicagoan who is proud to offer an array of innovative surgical and nonsurgical cosmetic procedures from his practice, SAC Plastic Surgery, in Oak Lawn, IL. Dr. Chowdhry is also the Chairman of Plastic Surgery at Advocate Medical Center, a 750-bed level I major metropolitan hospital and teaching facility, where he is well-respected by his peers. Dr. Chowdhry’s goal is to build trust with each patient so they feel comfortable candidly communicating their needs and cosmetic goals. By providing insight, knowledge, and skill, Dr. Chowdhry helps patients to make well-informed choices about their aesthetic goals, leading to beautiful, natural outcomes.
Dr. Chowdhry is a paid consultant for Solventum.
Chowdry_Current-Dialogues-in-Wound-Management_2026_Article-2
Background
Necrotizing soft tissue infections (NSTIs) frequently result in large, contaminated soft tissue defects following life-saving surgical debridement. While early operative intervention and antimicrobial therapy are essential, the subsequent phase of care—wound bed preparation and reconstruction—often determines long-term functional and reconstructive outcomes. Traditional approaches to managing these wounds often relies on open dressings with topical antimicrobials, frequent dressing changes, and repeated debridements, all of which may prolong hospitalization and delay definitive closure.
Solventum™ Veraflo™ Therapy has emerged as an adjunctive strategy for managing complex, contaminated wounds. By combining the mechanical benefits of negative pressure with intermittent instillation of topical solutions, Veraflo Therapy provides wound cleansing that solubilizes and removes infectious materials and wound debris, and promotes an environment for wound bed optimization for reconstruction.
Patient Overview
A 58-year-old female with type 2 diabetes mellitus developed a necrotizing soft tissue infection of the left groin requiring emergent surgical debridement. Following serial operative debridements by the general surgery service, a large open wound remained (Figure 1). At that stage, the patient was hemodynamically stable, the infection was controlled, and the primary clinical challenge had shifted from source control to preparing the wound for definitive closure.

Post-Debridement Wound Characteristics
After all nonviable tissue was removed, the left groin wound demonstrated exposed soft tissue, irregular contours, and moderate exudate. While gross necrosis had been addressed, the wound remained at risk for ongoing contamination due to its anatomic location and the patient’s underlying comorbidities. Ongoing wound management was required to:
- Reduce residual bioburden.
- Maintain a clean wound environment.
- Promote granulation tissue formation.
- Prepare for eventual reconstructive closure.
At this stage in the patient’s treatment course, several management pathways were considered.
Alternative Approaches to Wound Management
A traditional management of complex post-debridement wounds often relies on dressings and topical antimicrobial agents. However, this approach requires frequent dressing changes, prolonged periods of open wound care, and close inpatient monitoring. In addition, when topical antimicrobials are applied with standard dressings, consistent contact with the wound bed may not be maintained, an issue that is particularly problematic in deep or anatomically complex sites such as the groin.
Another option is to perform repeated operative debridements and washouts to maintain wound cleanliness. Although this approach is necessary in some cases, repeated trips to the operating room increase patient morbidity, extend anesthesia exposure, increase healthcare utilization, and may delay progression to reconstructive procedures.
In contrast, Veraflo Therapy offers a means of ongoing wound cleansing between operative interventions while maintaining a controlled wound environment.
Rationale for Veraflo Therapy
Veraflo Therapy was selected to optimize wound bed preparation while minimizing the need for further operative debridement. This modality allows for direct delivery of topical solutions into the wound bed with a user-controlled dwell time, ensuring consistent contact between the solution and the wound surface. The instillation cycles facilitate removal of solubilized debris, infectious material, and exudate during subsequent negative pressure phases.
Importantly, negative pressure therapy promotes wound contraction and supports vascular ingrowth through microdeformation of the wound bed. These effects contribute to progressive wound contraction and robust granulation tissue formation—key prerequisites for successful reconstruction.
In this case, Veraflo Therapy served not as a substitute for surgical debridement, but as an adjunct once adequate source control had been achieved, allowing the wound to progress efficiently toward closure.
Intervention
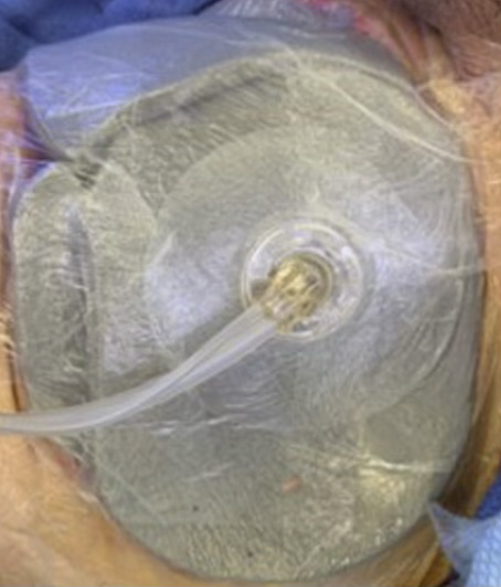
After the series of debridements was completed, Veraflo Therapy was initiated using Solventum™ Veraflo Cleanse Choice™ Dressing (Figure 2). The therapy was administered over two sequential treatment periods of three days each. Dakins solution (1/8 strength) was instilled into the wound bed with a 10-minute dwell time, followed continuous negative pressure at -125 mmHg for 2 hours. The dressing conformed well to the irregular wound geometry of the groin, facilitating uniform instillation and effective negative pressure across the wound surface. Dressing changes occurred every 2 days.
During therapy, the wound demonstrated progressive improvement without clinical evidence of recurrent infection. Additional operative debridement was not required, and dressing changes were performed in a controlled manner per institutional protocol.
Clinical Progress and Wound Bed Optimization
Over the course of Veraflo Therapy use, the wound exhibited decreased exudate, improvements in tissue quality, and development of healthy granulation tissue (Figure 3). The wound’s dimensions progressively decreased, reflecting both wound contraction and tissue ingrowth. The surrounding soft tissue inflammation improved, and the wound bed reached a state suitable for definitive reconstruction.

By providing continuous wound management between operative interventions, Veraflo Therapy supported an efficient progression through the wound preparation phase avoiding unnecessary hospitalization extensions or exposing the patient to additional surgical procedures.
Reconstruction and Outcome
Once the wound had developed a stable, granulating bed, a split-thickness skin graft was performed to achieve definitive closure. The graft demonstrated excellent take without any complications. The patient was discharged home approximately one week after reconstruction.
At the two-week follow-up visit, the grafted site was fully epithelialized with closed and healed incisions, and no wound-related complications were observed (Figure 4).

Discussion
The management of large post-debridement wounds following NSTI often involves a prolonged and resource-intensive phase of care. Without advanced wound-care modalities, patients may require extended periods of open wound management, necessitating frequent dressing changes and repeated operative interventions.
Veraflo Therapy offers several advantages in this setting. By combining negative pressure–induced wound contraction and vascular ingrowth with direct instillation of topical solutions, this modality supports efficient wound bed preparation. Its ability to maintain consistent contact between topical agents and the wound surface distinguishes Veraflo Therapy from standard open dressing methods and may reduce the need for repeated surgical debridement.
In this case, Veraflo Therapy with Veraflo Cleanse Choice Dressing facilitated timely progression from infection control to reconstruction, ultimately enabling early definitive closure with favourable outcomes.
Key Teaching Points
- Post-debridement wound management is a critical determinant of outcomes following NSTI.
- Traditional approaches such as open dressings and repeated debridements may prolong time to achieve wound closure.
- Veraflo Therapy allows for continuous wound cleansing, consistent topical agent delivery, and supports the formation of granulation tissue.
- The negative pressure component of Veraflo Therapy supports wound contraction and vascular ingrowth, preparing wounds for reconstruction.
- Appropriate use of Veraflo Therapy may reduce the need for additional operative interventions and expedite definitive closure.
References
NOTE: Specific indications, contraindications, warnings, precautions and safety information exist for these products and therapies. Please consult a clinician and product instructions for use prior to application. Rx only.
As with any case study, the results should not be interpreted as a guarantee or warranty of similar results. Individual results may vary depending on the patient’s circumstances and condition.
©Solventum 2026. Solventum, and S logo are trademarks of Solventum or its affiliates. 3M and the 3M logo are trademarks of 3M. All other trademarks are owned by their respective owners.
