Dr. Misael C. Alonso is a board-certified Internal Medicine physician and certified wound specialist with over two decades of experience delivering compassionate, expert care across multiple settings. A native of Chicago, Dr. Alonso earned his medical degree from the University of Illinois at Chicago College of Medicine in 1999. He completed his residency in Internal Medicine at Los Angeles County Hospital + University of Southern California in 2003. Driven by a commitment to service, Dr. Alonso joined the United States Air Force Reserve from 2001 to 2009 during his training, ultimately settling in Arizona near Luke Air Force Base. In 2003, he began practicing hospital medicine with the Arizona Medical Clinic, which later became part of the Banner Medical Group in 2007. In 2011, Dr. Alonso established his own practice, MCA Medical, PLLC, providing high-quality medical care to patients in skilled nursing facilities, group homes, and private residences throughout Arizona. In addition, Dr. Alonso provided locum tenens coverage at various hospitals in Arizona and Illinois until 2019. From this experience, Dr. Alonso gained an extensive experience in managing complex acute and chronic conditions. His longstanding interest in wound care led him to specialize in wound care focusing on chronic non-healing venous and diabetic wounds, pressure injuries, postsurgical wound complications and/or dehiscence. Dr Alonso is a paid consultant for Solventum.
Alonso_Current-Dialogues-in-Wound-Management_2026_Article-3
Patient and Diagnosis
A 44-year-old male with a medical history significant for morbid obesity and uncontrolled type 2 diabetes mellitus presented with right sided groin and abdominal pain which prompted hospital admission. The patient was subsequently diagnosed with Fournier’s gangrene complicated by severe sepsis, with cultures identifying group B Streptococcus as the causative pathogen. Additional diagnoses included severe protein-calorie malnutrition and vitamin D Deficiency.
Contrast-enhanced computed tomography of the abdomen/pelvis demonstrated findings of cellulitis/panniculitis associated with extensive subcutaneous emphysema and adjacent stranding extending from the right inguinal region along the upper right lateral thigh and the caudal aspect of the right lateral abdominal wall pannus. No subfascial gas was identified deep to the rectus abdominis muscle to suggest necrotizing fasciitis; however, the presence of a gas forming infection could not be excluded.
Prior to wound care consultation, the patient underwent two operative interventions. The first procedure consisted of extensive sharp excisional debridement including skin, subcutaneous tissue (including adipose tissue), muscle, and fascia, with a total debrided surface area of approximately 1,750 cm2. A second procedure was subsequently performed, consisting of further debridement of the lower pelvis, including the right groin, and right lower abdominal wall, with placement of Solventum™ Veraflo™ Therapy over the abdominal wound. A wound care consultation was requested to assist with implementing Veraflo therapy using a hypochlorous acid solution.
Initial Application of Veraflo Therapy
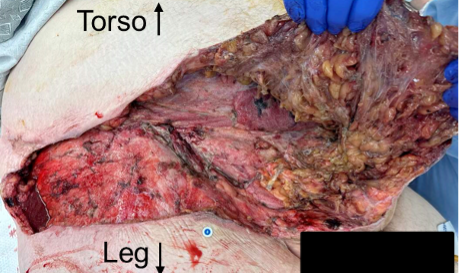
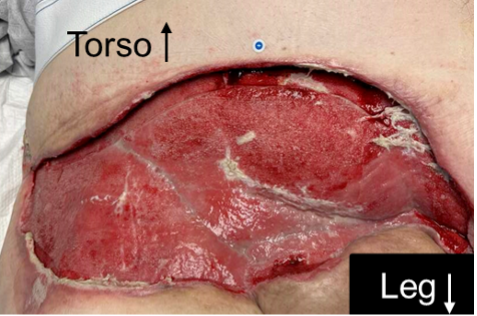
On Day 1, the patient underwent irrigation and debridement of the right groin and abdominal wall (Figure 1), followed by application of Veraflo Therapy. On examination, the wound measured 22.2 cm in length, 47.3 cm in width, and 12.0 cm in depth, with exposed necrotic muscle and necrotic subcutaneous adipose tissue. A large volume of serous drainage with a mild odor was noted, and the wound bed demonstrated 1–25% slough. The periwound skin exhibited edema and erythema and showed clinical signs and symptoms consistent with infection. Both systemic and topical antibiotics were prescribed.
Non-contact fluorescence imaging (MolecuLight i:X™, MolecuLight Corp, Pittsburgh, PA) was done to evaluate for the presence and location of pathogenic bacterial burden and demonstrated several areas of red fluorescence along the adipose tissue underneath the anterior abdominal wall, consistent with bacterial contamination. Near-infrared spectroscopy (Snapshot NIR, Kent Imaging, Calgary, AB, Canada) revealed adequate oxygenation within the wound bed; however, total hemoglobin levels were elevated, consistent with hyperemia secondary to inflammation and/or infection.
Veraflo therapy was delivered using a Solventum™ V.A.C.® Ulta™ Therapy Unit with intermittent negative pressure set at -150 mmHg. A large Solventum™ Veraflo™ Cleanse Choice Complete™ Dressing was applied. A hypochlorous acid solution (150 mL) was instilled into the wound bed with a 20-minute dwell time, followed by 3.5 hours of continuous negative pressure at -150 mmHg. Dressing changes occurred every 2–3 days.
Treatment
On Day 2, the patient reported that he was doing well, but wound size and exudate volume exceeded the capacity of a single V.A.C.® Ulta™ Therapy Unit. The dressing was therefore changed. Wound examination demonstrated ongoing exposure of necrotic muscle and necrotic adipose tissue, with a large amount of serous drainage noted that had a mild odor. The wound bed continued to exhibit 1–25% slough, with no change in overall wound progression. The periwound skin exhibited edema and erythema, with persistent clinical signs consistent with infection. Local wound care measures were continued, and systemic, topical, and local antimicrobial therapies were prescribed.
Veraflo therapy was reapplied and administered using two V.A.C.® Ulta Therapy Units that were synchronized to function simultaneously. Large Solventum™ Veraflo Cleanse Choice™ Dressings were applied to the wound bed. No changes were made to the therapy parameters or dressing change frequency. Veraflo therapy was continued for 19 days. At each dressing change, surgical debridement was performed, followed by reapplication of Veraflo Therapy using the Veraflo Cleanse Choice Dressings using the same therapy parameters and dressing change frequency. By Day 19, the wound demonstrated marked improvement, with granulation tissue formation observed (Figure 2). At this time, wound dimensions measured 13.13 cm in length, 32.24 cm in width, and 5.8 cm in depth.
Non-contact fluorescence imaging was performed to evaluate the presence and location of pathogenic bacterial burden. Residual fluorescence was primarily localized to the left lower quadrant in areas of remaining slough. Overall, the fluorescence signal was reduced compared to prior imaging assessments.
On Day 21, Veraflo Therapy was discontinued, and the patient underwent abdominal excisional debridement. At that time, the wound measured 17.9 cm in length, 38.7 cm in width, and 6 cm in depth. A moderate amount of serous drainage was noted without associated odor.The patientreportedno woundpain, consistent with an insensate wound.
The wound bed demonstrated substantial healing progression, with 76–100% bright red granulation tissue, 1–25% slough, and 1–25% epithelialization, indicating overall improvement. Non-contact, real-time fluorescence imaging was performed to assess residual bacterial burden and confirmed eradication of bacteria following debridement and lavage. Subsequently, an acellular human reticular dermal allograft and amnion-chorion placental allograft were applied to the wound bed. Following graft placement, 3M™ Adaptic™ Non-Adhering Dressing was applied followed by Solventum™ V.A.C.® Therapy application as a bolster. Negative pressure therapy was delivered using two V.A.C.® Ulta Therapy Units set to continuous pressure at -150 mmHg. Large Solventum™ V.A.C.® Granufoam™ Dressings were utilized with dressing changes every 2–3 days. On Day 23, V.A.C.® Therapy was continued; however, one of the two therapy units was discontinued with ongoing wound management maintained using a single unit.
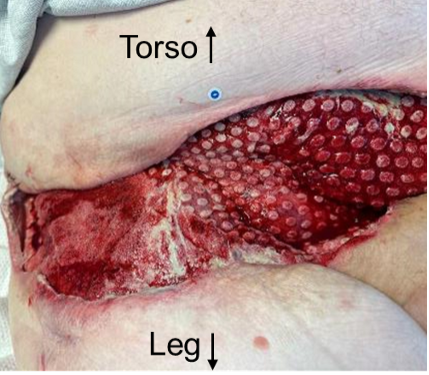
On Day 26, V.A.C.® Therapy was continued, and the patient reported he was doing well. At this time, wound dimensions measured 14.1 cm in length, 34.5 cm in width, and 8.5 cm in depth (Figure 3). Circumferential undermining was noted, extending from the 3:00 to 9:00 position measuring 6.2 cm, as well as additional undermining from the 9:00 to 3:00 position with a maximum distance of 3.8 cm. A moderate amount of sanguineous drainage was noted without associated odor. The patient reported no wound-related pain, consistent with an insensate wound. The wound bed continued to demonstrate favorable healing characteristics, with 76–100%, bright red granulation tissue, 1–25% slough, and 1–25% epithelialization. The periwound skin exhibited edema, scarring, and erythema; however, no clinical signs or symptoms of infection were observed.
Negative pressure therapy was delivered using one therapy unit using an extra-large V.A.C.® Granufoam™ Dressing and continuous negative pressure at -150 mmHg. Dressing changes occurred every 2-3 days.
On Day 33, the wound measured 15.9 cm in length, 37.7 cm in width, and 4.5 cm in depth. Undermining was present from the 3:00 position to the 8:00 position, with a maximum distance of 3.8 cm, with additional undermining noted from the 8:00 position to the 3:00 position with a maximum distance of 3.1 cm. A moderate amount of sanguineous drainage was noted with no associated odor. The wound bed continued to demonstrate favorable healing characteristics, with 76–100% bright red granulation tissue, 1–25% slough, and 1–25% epithelialization. The periwound skin exhibited edema, scarring and erythema; however, no clinical signs or symptoms of infection were noted. V.A.C.® Therapy was continued with the previous therapy parameters.
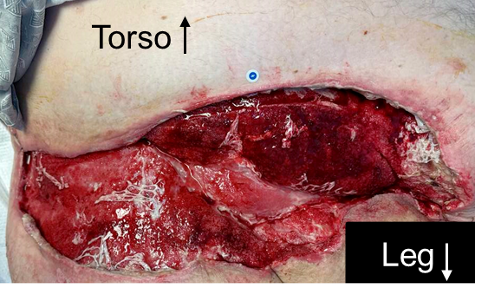
On Day 36, a non-contact, real-time fluorescence imaging was performed to assess the presence and location of pathogenic bacteria in the wound bed and periwound area. Fluorescence imaging demonstrated red fluorescence within the wound bed and periwound tissues, consistent with a high bacterial burden exceeding 104 colony forming units/gram (CFU/g). The patient subsequently underwent sharp debridement, with removal of adipose tissue, dermis, epidermis and subcutaneous tissue along with devitalized tissue, biofilm, exudate, fibrin and slough. Fluorescence imaging was repeated post-cleansing and debridement and demonstrated reduction or elimination of pathogenic bacteria confirmed by the absence of red or cyan fluorescence signals. Post debridement wound measurements were 18.1 cm in length, 35.3 cm in width, and 2.2 cm in depth (Figure 4). Undermining was noted from the 3:00 position to the 9:00 position with a maximum distance of 2 cm, with additional undermining from the 9:00 position to the 3:00 position, with a maximum distance of 1.1 cm. A moderate amount of sanguineous drainage was noted with no associated odor. Following completion of debridement and reassessment, V.A.C.® Therapy was reapplied.
- Figure 4 . Wound appearance on Day 36 (10 days after allograft application). Image courtesy of Misael C. Alonso, MD, FACP, CWSP, FAPWCA
Follow-up
On Day 38, the patient was discharged to home with home health services in place. Ongoing wound management included scheduled follow-up at the wound care clinic for continued V.A.C.® Therapy dressing changes. Discharge to an alternate care facility was not feasible due to the size and complexity of the wound.
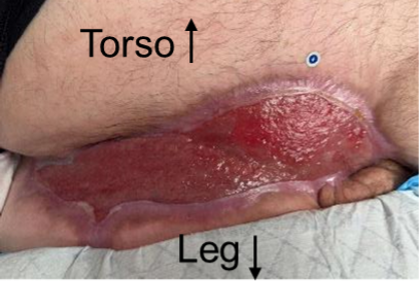
At outpatient follow-up on Day 48, the wound measured 12.2 cm in length, 29.6 cm in width, and 0.3 cm in depth, with 0.8 cm of undermining (Figure 5). The patient declined surgical closure and hyperbaric oxygen therapy. Consequently, the wound was left to heal by secondary intention.

- Figure 5 . Wound appearance 48 days after presentation. Image courtesy of Misael C. Alonso, MD, FACP, CWSP, FAPWCA
On Day 76, the patient underwent surgical debridement. The wound measured 9.3 cm in length, 30.5 cm in width, and 0.2 cm in depth (Figure 6). Given the degree of wound improvement, V.A.C.® Therapy was discontinued. Standard wound care dressings were initiated, with dressing changes performed once per week. Approximately 2.5 months after presentation, the wound measured 5.2 cm in length, 22.6 cm in width, and 0.1 cm in depth, with re-epithelialization observed (Figure 7). The wound continued to demonstrate healing by secondary intention (Figure 8). At approximately 11 months after presentation, wound closure had sufficiently progressed, and the patient was discharged from the wound care clinic.


Images courtesy of Misael C. Alonso, MD, FACP, CWSP, FAPWCA
Clinician Experience
In this large, complex abdominal wound, wound care required the use of multiple negative pressure therapy devices. Initially, the wound was managed with Veraflo Therapy to cleanse the wound and solubilize infectious material and devitalized tissue. Once the wound no longer required cleansing, treatment was stepped down to V.A.C.® Therapy to remove exudate and infectious materials while promoting granulation tissue development. The wound was left to heal by secondary intention and treatment was stepped down to standard of care wound dressings once the wound size and exudate level decreased, and the wound bed filled with healthy granulation tissue. The complexity of the wound did cause challenges throughout treatment. Two therapy units were required for both Veraflo Therapy and a portion of V.A.C.® Therapy use due to the high level of exudate, while the size and complexity of the wound made it difficult to discharge the patient from the hospital to a long-term wound care center or home health services. Despite these challenges, the use of Veraflo Therapy, V.A.C.® Therapy, and wound care dressings in this patient resulted in wound size reduction, granulation tissue development, and re-epithelialization.
References
Patient data and images courtesy of Misael C. Alonso, MD, FACP, CWSP, FAPWCA.
NOTE: Specific indications, contraindications, warnings, precautions and safety information exist for these products and therapies. Please consult a clinician and product instructions for use prior to application. Rx only.
As with any case study, the results should not be interpreted as a guarantee or warranty of comparable results. Individual results may vary depending on the patient’s circumstances and condition.
©Solventum 2026. Solventum, and S logo are trademarks of Solventum or its affiliates. 3M and the 3M logo are trademarks of 3M. All other trademarks are owned by their respective owners.
