
Liz McElroy is a Nurse Practitioner in Wound, Ostomy, and Continence Care at the Reading Hospital in West Reading, PA. She graduated from Gwynedd Mercy University with her MSN in Adult Nurse Practitioner in 2009, became a Certified Wound Specialist (CWS) in 2010, and certified in Wound, Ostomy, and Continence (CWOCN) in 2012. She serves as an in-patient wound, ostomy, and continence specialist for a 700+-bed Level I Trauma Center. She focuses on care of the perioperative, post-operative, cardiac and critical care patients, with an interest in nursing and physician education and V.A.C. VERAFLO™ Therapy.
McElroy_Current Dialogues in Wound Management_2019_Special Spring Edition
NOTE: As with any case study, the results and outcomes should not be interpreted as a guarantee or warranty of similar results. Individual results may vary depending on the patient’s circumstances and condition.
Negative pressure wound therapy (NPWT) has been a staple in complex wound management for over two decades now. As I entered my career as a graduate registered nurse at a small community hospital, I had my first experience using NPWT on complex wounds. I had no prior exposure to this therapy during my nursing training. I can remember that it seemed so complex when I first saw the kit, but luckily I had a mentor who did a great job of showing me the ropes. As I advanced through my nursing career, I gained experience with NPWT; however, the wound care team or the Certified Wound Ostomy Continence Nurse (CWOCN) was consulted for application and management of the more complex wounds. Years later when I came into the role of a Certified Wound Specialist (CWS) and CWOCN, I found that I was the person that others turned to for complex wounds.
Occasionally, when I received a consult for a complex wound, the physician would ask for a dressing recommendation because the physician felt a wound was “un-vac-able.” After a professional conversation with the consulting physician, I observed that there were four common themes that distinguished these complex wounds from non-complex ones:
 Figure 1. Example of a complex V.A.C. VERAFLO™ Therapy application on the hand.
Figure 1. Example of a complex V.A.C. VERAFLO™ Therapy application on the hand.
1) Wound location (i.e., close to the rectum, groin, or perineum);
2) Large wounds;
3) Wounds with multiple contours;
4) Wounds with a less than favorable periwound skin condition.
The providers often wanted to use NPWT, but the perceived complexities of utilizing the therapy seemed too challenging, and they did not want to fail. I took great pride in being able to apply NPWT to many of these complex wounds. However, I never came to the bedside without my pockets packed full of tricks. Over the years, with clinical and industry support, I found a playbook of wound care techniques that has left not only my service, but the providers who consulted our service, confident in the therapy they wanted and therapy they felt would be best for their patient.
 Figure 2. Example of a complex wound geography with V.A.C. VERAFLO™ Therapy on the hand
Figure 2. Example of a complex wound geography with V.A.C. VERAFLO™ Therapy on the hand
What are some of my recommendations on using NPWT with complex wounds and their complex geometries? How does NPWT with instillation and dwell time or V.A.C. VERAFLO™ Therapy affect those recommendations? V.A.C. VERAFLO™ Therapy has been shown to be an advanced therapy to help manage complex wounds, especially in contaminated wounds or wounds requiring further wound bed preparation.1 In my clinical experience, there are some basic rules to follow, with room for the clinician to incorporate the unique needs of the patient, wound, and clinical setting allowing for customization of the therapy settings and application. Instillation therapy is often viewed as a therapy that could increase the risk of leakage alarms. Certainly, when a good seal is questionable, to add the instillation of a solution makes that therapy seem impossible. However, with appropriate periwound skin preparation, use of accessory products, and innovative application techniques, the impossible is often very possible.
What is in my toolbox? The four major items are: skin protectant, barrier rings, drape application techniques, and settings. Skin preparation is key. A no-sting skin preparation solution is included with every V.A.C. VERAFLO™ Therapy kit for good reason. Once the periwound is appropriately dry, the application of the no-sting skin preparation solution will help with the adhesion of the drape. In my experience, this skin preparation step allows the wound cleansing solution to be instilled to the wound edge without causing a lifting of the drape. When the traditional no-sting skin preparation is not enough, there are additional options, such as the use of a cyanoacrylate, mastisol, or benzoin.
When it comes to wound location, wounds close to the groin, rectum, and perineum are often challenging to achieve or maintain a good seal, especially in the presence of incontinence. Whenever I apply NPWT in the groin or posterior trunk, I use barrier rings, skin protectant, and stoma paste. I also typically bridge away from these areas to keep the tubing away from pressure points. The use of barrier rings has proven to be extremely beneficial in my practice. Barrier rings are made with pectin-based, hydrocolloid-type ingredients, although composition varies by brand. They are moldable and customizable to
 Figure 3. Example of complex geography near the groin.
Figure 3. Example of complex geography near the groin.
meet clinician and patient needs.2 The pectin is the same substance used in jams and jellies. With the addition of pectin, the liquid thickens and creates a gel. When using barrier rings, the rings will often turn light in color when they encounter a liquid. They swell and create a “turtle neck” to prevent leaks of any liquid. This inhibits liquid from getting in (e.g., incontinence) and inhibits any liquid from getting out (e.g., the topical wound instillation solution). When applying the barrier rings or paste products, it is important to place them within 0.5 cm from the wound edge. If applied directly on the edge, the product may migrate into the wound when NPWT is turned on. When utilizing V.A.C. VERAFLO™ Therapy, I prefer to use the barrier rings instead of the paste, as I find it easier to remove the barrier rings at the next dressing change.
 Figure 4. V.A.C. VERAFLO™ Therapy on a complex wound close to the groin.
Figure 4. V.A.C. VERAFLO™ Therapy on a complex wound close to the groin.
Table 1 lists the pastes and barrier products (not inclusive) I have used in my practice. Drape application technique can make a difference in maintaining a seal that is needed with NPWT. Generally, with NPWT, the less overlapping of drape(s), the less likelihood of a trigger for a leak alarm. However, when the wound area is large, the clinician must use multiple pieces of drape to ensure a good seal. If a larger sheet of drape is used and there is a large wound area, this could lead to gaps between the skin and the drape, a phenomenon I refer to as tenting. When there are lots of hills and valleys, I would recommend a technique that I refer to as shingling. Shingling occurs when the clinician cuts multiple strips of drape and overlaps them by 50%. When a contractor applies shingles to a roof, it is for the purpose of keeping the elements (rain, ice, snow, etc.) on one side, and the other side dry. The same principle can be applied to the use of V.A.C. VERAFLO™ Therapy. When utilizing this technique, there is less risk for tenting, so the drape stays in good contact with the periwound skin, despite there being a large wound area. Care should be taken at the time of application to stretch the skin as flat as possible to prevent any wrinkles.
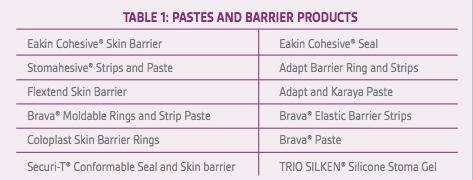
 Figure 5. Scrotal wounds can be a challenge with application.
Figure 5. Scrotal wounds can be a challenge with application.
Another technique used, especially on the distal foot, is to encompass the toes in the drape to “shrink wrap” them. When there is a wound between the toes or at the metatarsal head,
 Figure 6. Use of barrier rings and shingling drape application helps to obtain a good seal.
Figure 6. Use of barrier rings and shingling drape application helps to obtain a good seal.
obtaining a good seal can prove challenging. I would apply an absorptive dressing such as a silver alginate between the toes, use a barrier ring around the periwound, and apply the drape from the plantar aspect to the dorsal aspect, which would encompass all the toes. Certainly, the clinician needs to consider sensation and weight-bearing status when determining if this technique could be utilized.
 Figure 7. When applying drape over the toes, be sure to use an absorptive dressing between them.
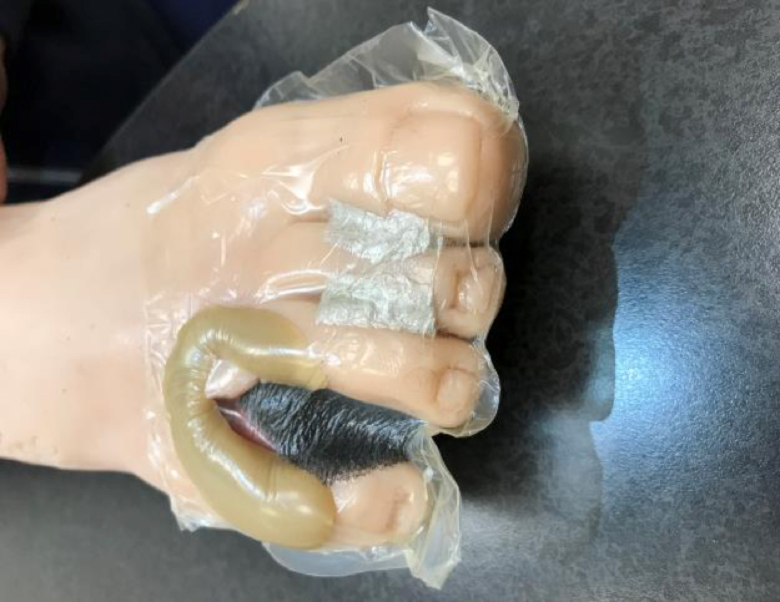
Figure 7. When applying drape over the toes, be sure to use an absorptive dressing between them. Figure 8. Drape application when “shrink wrapping” the toes.
Figure 8. Drape application when “shrink wrapping” the toes.

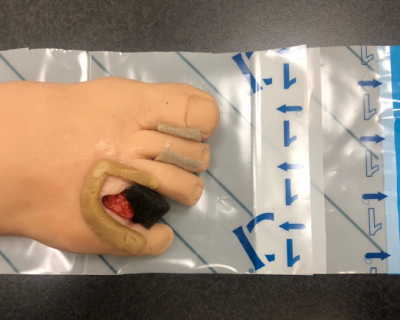
 Figure 9. Shrink wrapping the toes to maintain a good seal with interdigital lesions.
Figure 9. Shrink wrapping the toes to maintain a good seal with interdigital lesions.
Of course, in the presence of too much liquid, the barrier rings and the drape can fail, which is why the settings on V.A.C. VERAFLO™ Therapy can be important to allow a successful therapy. Overfilling the foam dressing will cause any dressing to fail. When there is a high concern for a leak, the clinician can lessen the volume of instillation and lessen the dwell time to help prevent any leaks.
 Figure 10. Use of barrier ring in a complex foot wound.
Figure 10. Use of barrier ring in a complex foot wound.
When the clinician takes the time to prepare the periwound skin and uses the appropriate accessories to apply the V.A.C. VERAFLO™ Therapy, a good seal can typically be achieved. While wound care is both an art and a science, highly geometrical wounds tend to allow clinicians to use their artistic side, in addition to merging the evolving science on this advanced wound therapy.
 Figure 11. Application of drape to protect incision line and prevent leaks.
Figure 11. Application of drape to protect incision line and prevent leaks. Figure 12. Intact V.A.C. VERAFLO™ Therapy dressing on a complex foot wound.
Figure 12. Intact V.A.C. VERAFLO™ Therapy dressing on a complex foot wound.


References
1.Gupta S, Gabriel A, Lantis J, Téot L. Clinical recommendations and practical guide for negative pressure wound therapy with instillation. Int Wound J. 2016;13:159-174. doi: 10.1111/iwj.12452.
2.McKanna M, Geraci J, Hall K, et al. Clinician panel recommendations for use of negative pressure wound therapy with instillation. Ostomy Wound Manage. 2016;62(4):S3-S14.
3.Kim PJ, Applewhite A, Dardano AN, et al. Use of a novel foam dressing with negative pressure wound therapy and instillation: Recommendations and clinical experience. Wounds. 2018;30(3 Suppl):S1-S17.
