
Pablo Sibaja received his premedical education in the fields of biomedical engineering and zoology at Iowa State University and later enrolled at the medical school of the Universidad Autonoma de Centroamerica in San José. He completed his residency program in General Surgery at the University of Costa Rica in Hospital México and later received further training in the field of Trauma and Surgical Intensive Care within a joint program of cooperation held by the Oregon Health Sciences University stationed at Portland Oregon. He is currently Professor of Surgery and National Program Coordinator for the Residency of General Surgery of the University of Costa Rica and the Social Security of Costa Rica. He is Chief of the Surgical Intensive Care Unit at the Hospital Mexico, Costa Rican Social Security, San José, Costa Rica. He has been an invited speaker to numerous meetings in the Latin American region and has delivered over 100 lectures in this capacity. He is part of the editorial board for the medical journal of the University of Costa Rica and has authored chapters for five books published in Spanish and Portuguese and several journals in Latin America.

Dr. Alfredo Sanchez completed his medical training at Universidad San Judas Tadeo in San Jose, Costa Rica. Dr. Sanchez is one of the lead researchers associated with Universidad San Judas Tadeo and has published various papers regarding abdominal sepsis. His current clinical and research interests include negative pressure wound therapy in the open abdomen.

Dr. Milagros González completed her pre-medical training at Mississippi College and her medical training at Universidad San Judas Tadeo in Costa Rica. She is the medical coordinator for the Casa del Socorro Clinic.
NOTE: As with any case study, the results and outcomes should not be interpreted as a guarantee or warranty of similar results. Individual results may vary depending on the patient’s circumstances and condition.
ABSTRACT
Severe intra-abdominal sepsis is a potentially lethal condition requiring complex medical and surgical treatments. In special cases, due to the underlying conditions of patients, special care is required when dealing with complex and uncommon complications that lead up to abdominal sepsis. Negative pressure wound therapy (NPWT) appears to be the ideal temporary abdominal closure technique and the ABTHERA™ Open Abdomen Negative Pressure Therapy system is an optimal choice for its delivery. The preservation of biological meshes in patients with abdominal sepsis appears to be an adequate strategy since the mesh does not become an added source of infection.
We present the case of a 51-year-old male who, after suffering a work-related fall, had a perforated viscus that was managed with a colostomy and an incisional hernia. During the colostomy reversal procedure a biological mesh was put in place. Afterward, the patient suffered an anastomotic leak on two different occasions and developed a severe abdominal infection requiring management with NPWT. The patient had a good response to treatment and the abdominal mesh did not require removal.
INTRODUCTION
The management of the open abdomen (OA) has been widely studied during the past three decades and has undergone significant changes. There have been many different modalities of Temporary Abdominal Closure (TAC) devices, such as zippers, meshes, dynamic retention, polyvinyl covers and negative pressure devices. Additionally, there are different conditions that can be addressed with an open abdomen, such as abdominal hypertension1, abdominal compartment syndrome, pancreatitis, loss of abdominal wall and the need for a “second look” surgery2. Severe sepsis (SS) as defined by Dellinger3(organ dysfunction and hypoperfusion concomitant to infection) is the main causes of death in non-coronary ICUs4. In the United States of America the incidence of SS is 300 cases per 100 000 population5 with approximately 934,000 cases diagnosed every year and 215,000 deaths. In Europe, the number of deaths per year attributed to SS is 150,0006,7.The most frequent cause of severe sepsis in surgical ICU patients is peritonitis
Certain characteristics are linked to a higher mortality in patients with SS such as delayed medical attention, advanced age (≥65 years), malnourishment and a weakened immune response9–11.Overall, current mortality rates for intra-abdominal sepsis are 10.5%12. Advances in antibiotic therapy, renal and respiratory support, as well as newer and more effective forms of surgical techniques have all contributed to the reduction of morbidity and mortality in cases of SS.The application of “damage control” surgery13 has yielded positive results in the management of non-trauma patients as well14. Different OA techniques have been used in this context, in which, negative pressure therapy appears to be the modality of choice
The risk of abdominal meshes being infected is about 3- 13%, although this varies greatly and is influenced by the use of different materials. The use of newer biological meshes appear to have gained adoption both as a replacement for infected synthetic meshes, as well as the material of choice in patients who have a higher risk of developing a contaminated abdominal cavity, such as in our current case study.
We report the case of a 51-year-old male who suffered an intestinal perforation through a work-related injury that required a colostomy to be performed. Ten months later, during the colostomy reversal procedure, the patient had an anastomotic leak that led to an intra-abdominal sepsis that was managed with an open abdomen technique utilizing NPWT delivered via the ABTHERA™ Open Abdomen Negative Pressure Therapy system and a later abdominal wall reconstruction with a biological mesh placement (STRATTICE™ Reconstructive Tissue Matrix; Allergan, NJ). Subsequently, the patient had another anastomotic leak that required a second round of NPWT that allowed the mesh to be preserved.
CASE REPORT
A 51-year-old male with no past medical history presented to us after having suffered a work-related fall, which led to an intestinal perforation and an associated abdominal sepsis.The initial infection was treated with an open abdomen and twelve surgical lavages of the abdominal cavity; the patient underwent a Hartmann colostomy (also known as a proctosigmoidectomy), after which, he was discharged.
Ten months after the initial treatment, the patient was admitted for an elective colostomy reversal. During the procedure, multiple peritoneal adhesions and a fixed left colon was observed. The lateral/end anastomosis was achieved with some difficulty. On post-operative day # 5 fecal matter was observed through one of the surgical wounds and an open exploration of the abdomen was performed, where a dehiscence of the intestinal anastomoses was observed. The patient was treated with an OA and NPWT delivered via the ABTHERA™ Open Abdomen Negative Pressure Therapy system (figure 1-2), with continuous pressure applied at -125 mmHg and dressing changes every 48 hours.
After the third cycle, the patient’s clinical condition was stable and fascia closure was performed. Due to the presence of a large ventral hernia, a biological mesh (STRATTICE™ Reconstructive Tissue Matrix; Allergan, NJ) was used (Figure 3).On the POD# 4 following fascia closure, fever and wound cellulitis was observed. The wound exploration showed signs of sepsis and the abdominal cavity was reopened. During the exploration, it was observed that the anastomoses had leaked once again, therefore V.A.C.® Therapy utilizing V.A.C.® GRANUFOAM SILVER™ Dressing was initiated over the surgical wound with the biologic mesh (Figure 4). Two dressing changes every 48 hours were performed. Due to the recurrent dehiscence of the colonic sutures, the initial colostomy was reinstated. During this process it was observed that the mesh was intact and that there was no need to remove it.
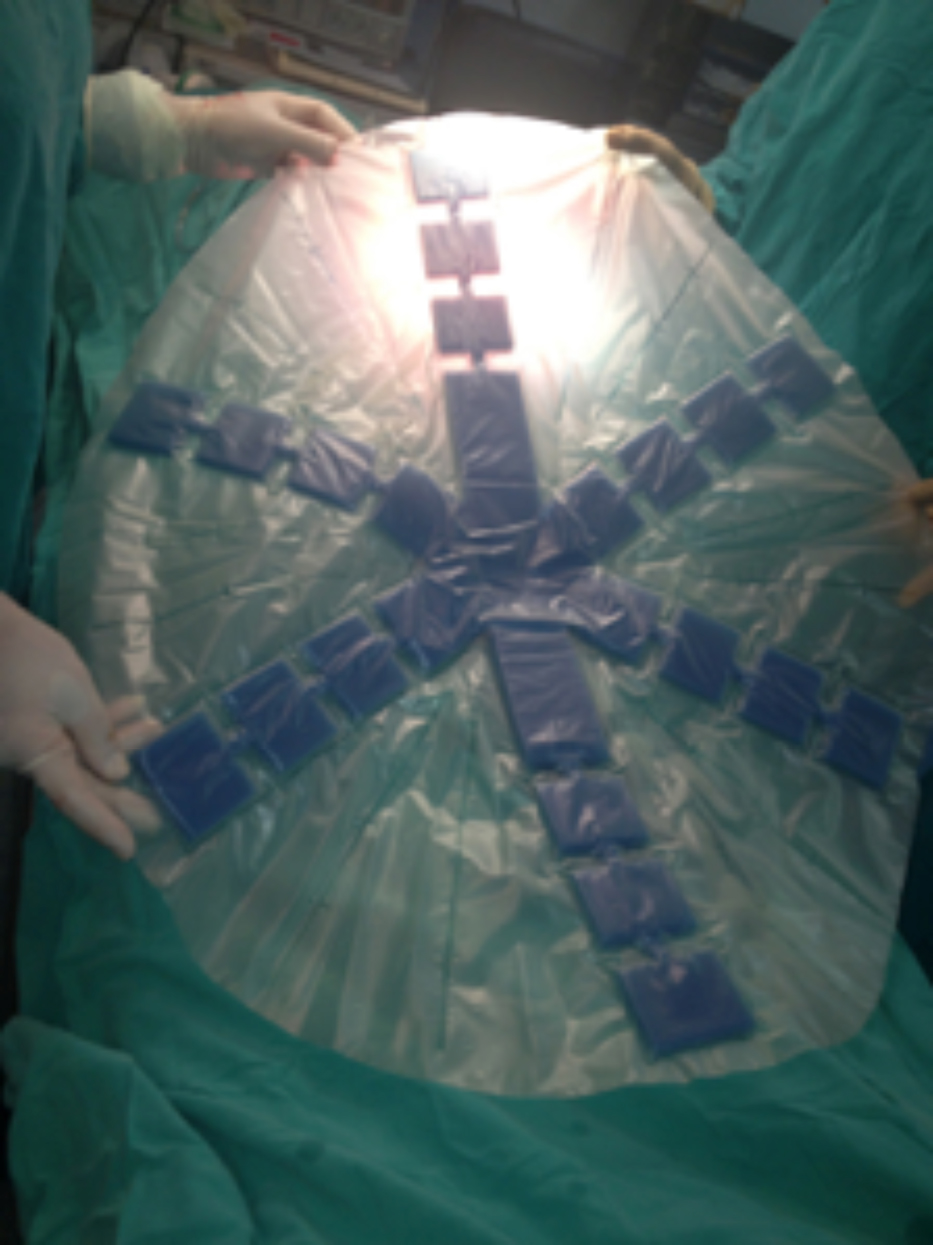

Figures 1-2: Negative Pressure Wound Therapy via the ABTHERA™ Open Abdomen Negative Pressure Therapy system utilized to help manage the patient’s abdominal sepsis. Note the external foam covering of the colostomy wound after initial reversal.
 Figure 3: Biological mesh fitted to treat the ventral hernia caused by the Open Abdomen approach.
Figure 3: Biological mesh fitted to treat the ventral hernia caused by the Open Abdomen approach.

The patient had a satisfactory outcome and was discharged. A three-week follow-up was performed where it was observed that the surgical wound had healed and there was no evidence of abdominal sepsis. (Figure 5).
DISCUSSION
Patients that require the use of an open abdomen approach have a high rate of ventral hernias, especially those in which primary fascia closure cannot be performed16 or the hernia is a planned outcome17. The use of different types of mesh materials have shown to be of great use in the treatment of these hernias18. Both synthetic and biological meshes have their benefits and downfalls. It appears that synthetics have a higher rate of complications19, especially when it comes to mesh related infections. The use of biological meshes, in conjunction with NPWT appears to be a good therapeutic strategy for abdominal sepsis in patients in which mesh preservation is to be performed
 Figure 4: Application of V.A.C.® Therapy with V.A.C.® GRANUFOAM SILVER™ Dressing over surgical wound.
Figure 4: Application of V.A.C.® Therapy with V.A.C.® GRANUFOAM SILVER™ Dressing over surgical wound. Figure 5: Closed abdomen with no signs of wound dehiscence or infection.
Figure 5: Closed abdomen with no signs of wound dehiscence or infection.


Our patient had multiple instances of abdominal sepsis that required management with an open abdomen, in the latter two events, the patient’s infectious foci was adequately treated with V.A.C.® Therapy placed over the surgical wound with the biologic mesh, but due to the recurrence of his anastomotic leak, the source of the infection was not fully addressed until the colostomy was reinstated.
This case exemplifies that maintaining the biological mesh, thus limiting surgical trauma on a patient with a previously addressed ventral hernia, while managing the abdominal infection with NPWT delivered via the ABTHERA™ Open Abdomen Negative Pressure Therapy system is a viable treatment option.
References
1.Batacchi S, Matano S, Nella A, Zagli G, Bonizzoli M, Pasquini A, et al. Vacuum-assisted closure device enhances recovery of critically ill patients following emergency surgical procedures. Crit Care [Internet]. 2009 [cited 2016 Jun 2];13(6):R194. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19961614
2. Coccolini F, Biffl W, Catena F, Ceresoli M, Chiara O, Cimbanassi S, et al. The open abdomen, indications, management and definitive closure. World J Emerg Surg [Internet]. 2015 [cited 2018 Jan 23];10:32. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26213565
3. Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med [Internet]. 2008 Jan [cited 2018 Jan 23];36(1):296–327. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18158437
4. Mayr FB, Yende S, Angus DC. Epidemiology of severe sepsis. Virulence [Internet]. 2014 Jan 1 [cited 2018 Jan 23];5(1):4–11. Available from: http://www.ncbi.nlm.nih.gov/pubmed/24335434
5. Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. [cited 2018 Jan 23]; Available from: https://s3.amazonaws.com/academia.edu.documents/7342771/angus_ccm_2001_1303.pdf?AWSAccessKeyId=AKIAIWOWYYGZ2Y53UL3A&Expires=1516730376&Signature=FONbmFCLsOO29tACsOHQcIoHCK4%3D&response-content-disposition=inline%3B filename%3DEpidemiology_of_severe_sepsis_in_the_Uni.pdf
6.Vincent J-L, Gerlach H. Fluid resuscitation in severe sepsis and septic shock: an evidence-based review. Crit Care Med [Internet]. 2004 Nov [cited 2016 Jun 2];32(11 Suppl):S451-4. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15542955
7. Dellinger RP. Cardiovascular management of septic shock. Crit Care Med [Internet]. 2003 Mar [cited 2016 Jun 2];31(3):946–55. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12627010
8. Weiss G, Steffanie W, Lippert H. Die Peritonitis – Hauptursache schwerer Sepsis auf chirurgischer Intensivstation. Zentralbl Chir [Internet]. 2007 Apr [cited 2018 Jan 23];132(2):130–7. Available from: http://www.ncbi.nlm.nih.gov/pubmed/17516319
9. Anaya DA, Nathens AB. Risk factors for severe sepsis in secondary peritonitis. Surg Infect (Larchmt) [Internet]. 2003 [cited 2016 Jun 2];4(4):355–62. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15012862
10. Solomkin JS, Mazuski JE, Bradley JS, Rodvold KA, Goldstein EJC, Baron EJ, et al. Diagnosis and Management of Complicated Intra‐abdominal Infection in Adults and Children: Guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis [Internet]. 2010 Jan 15 [cited 2016 Jun 2];50(2):133–64. Available from: http://cid.oxfordjournals.org/lookup/doi/10.1086/649554
11.Kaplan M, Onder A, Oguz A, Taskesen F, Aliosmanoglu I, Gul M, et al. The effective risk factors on mortality in patients undergoing damage control surgery. Eur Rev Med Pharmacol Sci [Internet]. 2013;17(12):1681–7. Available from: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&CSC=Y&NEWS=N&PAGE=fulltext&D=medl&AN=23832738
12. Sartelli M, Catena F, Ansaloni L, Coccolini F, Corbella D, Moore EE, et al. Complicated intra-abdominal infections worldwide: the definitive data of the CIAOW Study. World J Emerg Surg [Internet]. 2014 May 14 [cited 2018 Jan 23];9(1):37. Available from: http://wjes.biomedcentral.com/articles/10.1186/1749-7922-9-37
13. Rotondo MF, Schwab CW, McGonigal MD, Phillips GR, Fruchterman TM, Kauder DR, et al. “Damage control”: an approach for improved
14.14. Becher RD, Peitzman AB, Sperry JL, Gallaher JR, Neff LP, Sun Y, et al. Damage control operations in non-trauma patients: defining criteria for the staged rapid source control laparotomy in emergency general surgery. World J Emerg Surg [Internet]. 2016;11(1):10. Available from: http://www.wjes.org/content/11/1/10
15.Chiara O, Cimbanassi S, Biffl W, Leppaniemi A, Henry S, Scalea TM, et al. International consensus conference on open abdomen in trauma. J Trauma Acute Care Surg [Internet]. 2016 Jan 14 [cited 2017 Jun 27];80(1):173–83. Available from: http://content.wkhealth.com/linkback/openurl?sid=WKPTLP:landingpage&an=01586154-201601000-00026
16. Miller PR, Meredith JW, Johnson JC, Chang MC. Prospective evaluation of vacuum-assisted fascial closure after open abdomen: planned ventral hernia rate is substantially reduced. Ann Surg [Internet]. 2004 May [cited 2016 Jun 2];239(5):608-14-6. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15082964
17. Fabian TC, Croce MA, Pritchard FE, Minard G, Hickerson WL, Howell RL, et al. Planned ventral hernia. Staged management for acute abdominal wall defects. Ann Surg [Internet]. 1994 Jun [cited 2018 Feb 19];219(6):643-50-3. Available from: http://www.ncbi.nlm.nih.gov/pubmed/8203973
18. Stremitzer S, Bachleitner-Hofmann T, Gradl B, Gruenbeck M, Bachleitner-Hofmann B, Mittlboeck M, et al. Mesh Graft Infection Following Abdominal Hernia Repair: Risk Factor Evaluation and Strategies of Mesh Graft Preservation. A Retrospective Analysis of 476 Operations. World J Surg [Internet]. 2010 Jul 7 [cited 2018 Feb 20];34(7):1702–9. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20372901
19. van’t Riet M, van Steenwijk PJ de V, Bonjer HJ, Steyerberg EW, Jeekel J. Mesh repair for postoperative wound dehiscence in the presence of infection: is absorbable mesh safer than non-absorbable mesh? Hernia [Internet]. 2007 Oct 6 [cited 2018 Feb 20];11(5):409–13. Available from: http://www.ncbi.nlm.nih.gov/pubmed/17551808
20. Montgomery A, Kallinowski F, Köckerling F. Evidence for Replacement of an Infected Synthetic by a Biological Mesh in Abdominal Wall Hernia Repair. Front Surg [Internet]. 2015 [cited 2018 Feb 20];2:67. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26779487
