
Julie M. Robertson received a Bachelor of Science in Molecular and Cellular Biology from Texas A&M University and a PhD in Immunology from the University of Texas Graduate School of Biomedical Sciences in Houston. Following graduation, she became a post-doctoral fellow and a scientific writer for the laboratory of Dr. Judith James at the Oklahoma Medical Research Foundation. During her time in Oklahoma, Dr. Robertson gained valuable scientific and medical writing experience in the field of autoimmune disease through manuscript, abstract, poster, and grant writing. After leaving Oklahoma, Dr. Robertson became a medical writer at Acelity where she has helped health care professionals publish wound care manuscripts in peer reviewed journals.

Ricardo Martinez has worked in the Medical Device Industry for over 25 years in the areas of Product Development, Regulatory Affairs and Medical Information and Publications for distinguished companies such as Adeza Biomedical, Sunnyvale CA; SA Scientific and Acelity of San Antonio, TX. As the Sr Director of Medical Information and Publications for Acelity, Mr. Martinez leads an innovative team of Medical Information and Publication specialists that support a network of health care professionals (HCPs) from around the world. In his current work in Publications, Mr. Martinez assists HCPs to publish their medical findings and techniques in areas of wound care and regenerative medicine in various journals. Mr. Martinez holds a Master’s of Science degree from Texas A&I University, Kingsville, TX.
Robertson and Martinez_Current Dialogues in Wound Management_2019_Volume 5_Issue 1
Introduction
Diabetes affects millions of people in the United States (US) and incidence rates continue to increase. 1;2 Over the course of the disease, up to 25% of all diabetic patients will develop diabetic foot ulcers (DFUs).3 However, developing an effective treatment plan can be difficult. Previous DFU treatment algorithms did not contain updated treatment options currently available; as such, Blume and Wu recently updated and expanded the current Wagner DFU algorithm to include a multidisciplinary approach to patient care and treatment modalities.4 Here, we provide a summary of the Blume and Wu update to the DFU treatment algorithm.
PATIENT AND WOUND ASSESSMENT
A thorough patient and wound assessment is necessary for each patient visit4 and will help ensure that the development of DFUs are caught and treated early. A list of key items for the patient and wound assessment are shown in (Table 1).
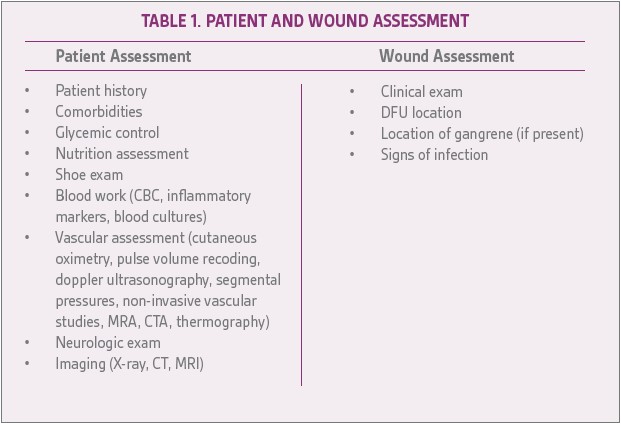
Adapted from Blume et al.4 CBC= complete blood count; MRA= magnetic resonance angiogram; CTA= computed tomography angiography; CT= computed tomography; MRI= magnetic resonance imaging
PREVENTATIVE CARE
If signs of calluses or uneven distribution of foot pressure is present, preventative care is necessary to help prevent the development of a DFU. 4 Blume et al recommends a multidisciplinary team consisting of a podiatrist, pedorthist, endocrinologist, vascular specialist, and primary care physician be involved with patient care. 4 Treatment recommendations included appropriate off- loading, diabetes education, and continued monitoring (Figure 1).
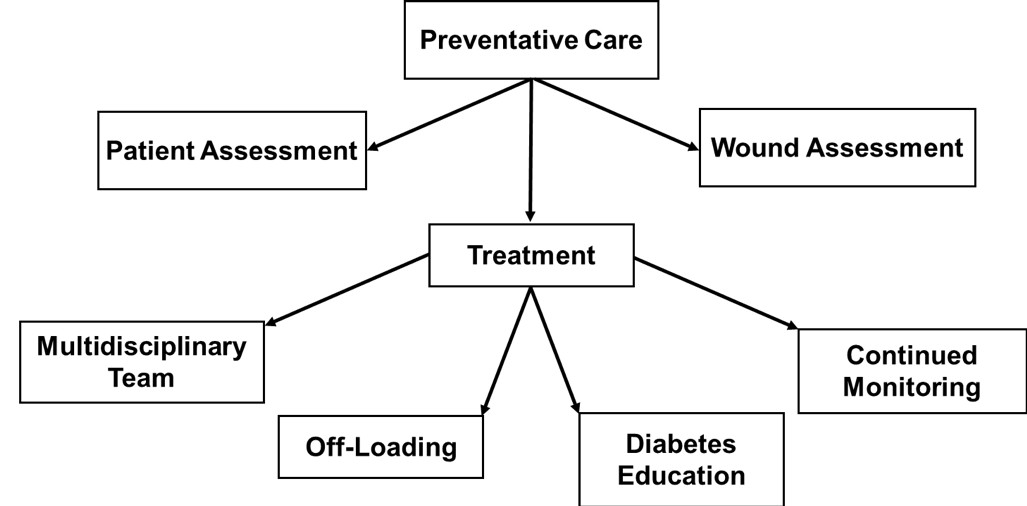
Figure 1. Preventative care algorithm. Adapted from Blume et al.
ACUTE/CHRONIC DFU
Acute/chronic DFUs can range from a superficial ulcer to a deep ulcer with tendon, ligament, joint capsule, and bone involvement with or without an infection.4 Patients may be in outpatient care throughout treatment. Diabetic education and a care team consisting of a podiatrist, pedorthist, endocrinologist, vascular specialist, interventional cardiologist, interventional radiologist, and wound care specialist were recommended.4 Treatment recommendations included debridement, advanced wound dressings, advanced wound therapy, skin grafting/skin substitutes, and off-loading (Figure 2). If infection is present, Infectious Diseases Society of America (IDSA) diabetic foot infection guidelines should be followed.
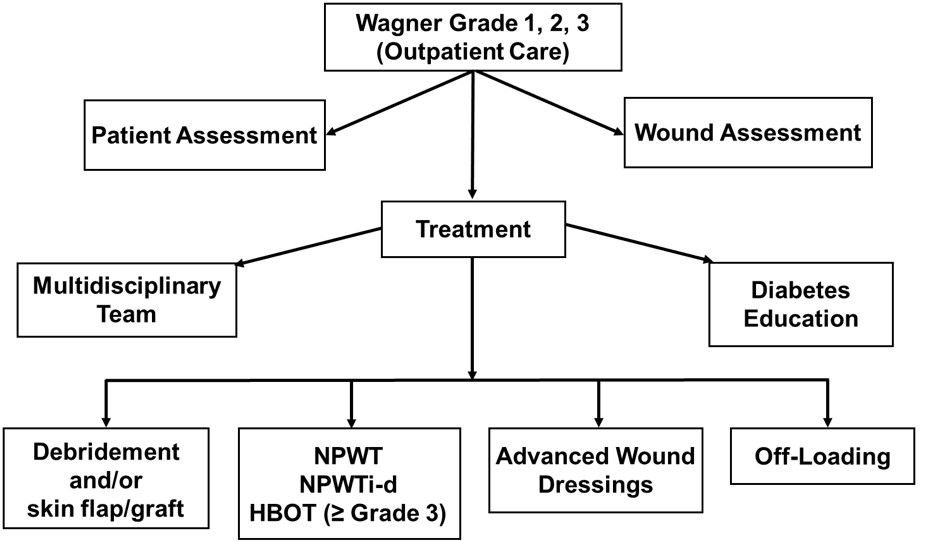
Figure 2. Treatment algorithm for Wagner Grade 1, 2, and 3 diabetic foot
ACUTE/URGENT DFU
Acute/urgent DFUs are severe (Wagner grade 3, 4, and 5) and can range from deep ulcer with infection, abscess, osteomyelitis, and joint sepsis to localized gangrene of the foot or more rarely gangrene of the entire foot.4Care for these severe DFUs is usually given in an inpatient setting. The recommended multidisciplinary care team included podiatry, pedorthic, orthopedic, vascular, infectious disease, wound care, endocrinology, interventional cardiology, interventional radiology, plastic surgery (if necessary) and diabetic education departments.4 Treatment should follow the IDSA diabetic foot infection guidelines.5 These urgent DFUs may require amputation (either local digit or foot/limb amputation). Post-surgical treatments should include advanced wound therapies, advanced wound dressings, and off-loading (Figure 3).
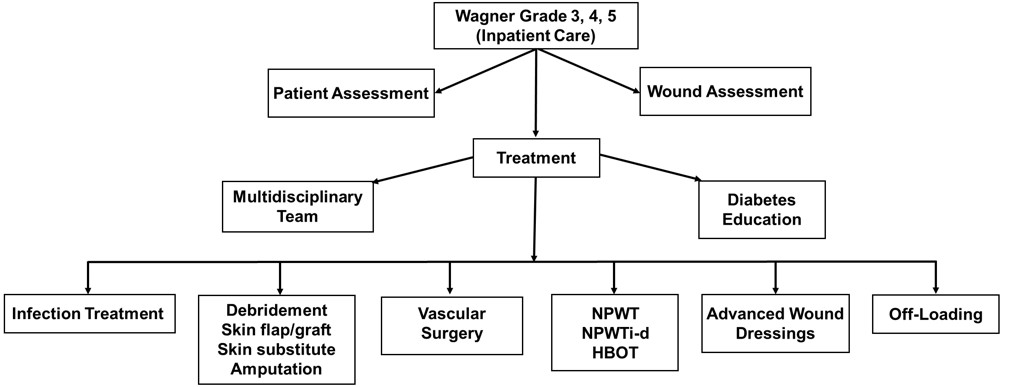
Figure 3. Treatment algorithm for Wagner Grade 3, 4, and 5 diabetic foot ulcers requiring inpatient care. NPWT= negative pressure wound therapy; NPWTi-d= negative pressure wound therapy with instillation and dwell time; HBOT= hyperbaric oxygen therapy. Adapted from Blume et al.
DISCUSSION
Blume and Wu provided an update for the Wagner grade DFU algorithm, which provided recommendations for preventative care through acute/urgent DFUs using currently available treatment modalities. Treatment of DFUs can be difficult as underlying patient comorbidities and lack of patient compliance can affect DFU healing. As clinicians will come across hard-to heal ulcers, Blume et al recommended that wound healing should be monitored at each stage of treatment and therapies changed if wound improvements are not observed after 2-3 weeks of treatment use.4 It was recommended that treatment for DFUs should start when a possible pre-ulcer is noticed as this prophylactic treatment may reduce development of more severe DFUs. The authors recommended a multidisciplinary care team for each DFU category, appropriate off-loading, and continuing diabetes education for all DFUs. As the DFU categories increased in severity, advanced wound dressings and advanced wound therapies optimized for the patient and the wound bed were recommended.4 The Wagner DFU algorithm from Blume and Wu updated and expanded the current Wagner DFU algorithm; however, principles from this algorithm may be expanded to other wound grading systems and wound types as multidisciplinary care and use of advanced technologies is beneficial for patients.
References
1. Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2014: Estimates of Diabetes and Its Burden in the United States. www cdc gov [serial online] 2014; Available from: Centers for Disease Control and Prevention. Accessed September 30, 2015.
2.Centers for Disease Control and Prevention. Diabetes Report Card 2014. www cdc gov 2015
3.Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. J Am Med Assoc 2005;293:217-228.
4.Blume P, Wu S. Updating the Diabetic Foot Treatment Algorithm: Recommendations on Treatment Using Advanced Medicine and Therapies. Wounds 2018;30:29-35.
5.Lipsky BA, Berendt AR, Cornia PB et al. 2012 infectious diseases society of america clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin Infect Dis2012;54:e132-e173.
