Professor EmeritusVirginia
Commonwealth UniversityRichmond,
VA
Ivatury_Current Dialogues in Wound Management_2015_Volume 1_Issue 2
INTRA-ABDOMINAL infections are a serious cause of mortality, ranging from 7.7% to 32.4% in subgroups with and without severe sepsis or septic shock at admission.1,2The pathogens responsible include the usual gram-negative, gram-positive, and anaerobic bacteria. In addition to prompt resuscitation and broad-spectrum antibiotic therapy, source control (removal) of contamination is the key for a successful outcome. This involves operative (open or laparoscopic) as well as nonoperative (e.g., interventional radiology) techniques.
In the majority of patients, source control may be achieved at the first procedure. In patients with established peritonitis from late presentation, missed diagnosis or delayed intervention, however, the infection may continue unabated after the initial procedure. This may lead to an uncontrolled immune response, severe sepsis, septic shock, and organ failure. In these patients, relaparotomy strategies may be required to control the abdominal source of infection. Open abdomen3-6 (nonclosure of fascia, temporary abdominal closure [TAC]) is a useful approach to achieve this goal. This review will briefly summarize some of the salient features of the open abdomen approach.
An open abdomen (nonclosure of fascia) approach may be required for abdominal sepsis for three reasons. First, many patients with severe sepsis or septic shock are profoundly unstable and are not optimal candidates for complex, prolonged operative interventions. Open abdomen allows for abbreviated laparotomy and staged reconstructions (so-called damage control, DC). Second, it facilitates repeated, easy access to extensive purulence that could not be eradicated at the initial procedure. Third, severe sepsis and septic shock need massive volume resuscitation. This may result in capillary leak and excessive fluid losses into the peritoneal cavity. All of these, together with marked bowel edema, precipitate increased intra-abdominal pressure and splanchnic hypoperfusion. Open abdomen may prevent some of these complications.
SEQUENTIAL THERAPIES INDAMAGE CONTROL AND OPEN ABDOMEN
Leaving the abdomen open constitutes the first phase of “damage control” (Part 1: initial laparotomy). Rapid source control of contamination by suturing, stapling, ligating, or excising perforation-bearing segments of bowel is the goal. Definitive repair, re-establishing intestinal continuity, stoma formation, and feeding ostomies are postponed to the next stage. The abdomen is closed by TAC only, without fascial suturing (open abdomen). Resuscitation is continued in the intensive care unit (ICU) (Part 2: ICU resuscitation).
After the abbreviated laparotomy, the focus now is on aggressive resuscitation in the ICU. The main goals are reversal of acidosis, hypothermia, and coagulopathy and euvolemia with restored end-organ perfusion, monitored by such basic end-points as vital signs, base excess, and serum lactate. Other goals at this juncture are prevention of volutrauma and barotrauma to the lung and the monitoring and control of intra-abdominal pressure. Once these parameters are optimized, the patient is returned to the operating room for definitive reconstruction of the bowel and/or ostomies (Part 3: subsequent laparotomy/definitive repair). In the majority of patients with abdominal sepsis, fascial closure is still undesirable, either due to excessive tension and/or incomplete evacuation of peritoneal purulence. Open abdomen is continued.
PART 4: SEQUENTIAL ABDOMINAL WALL CLOSURE
Closure of the abdominal wall fascia has evolved over the past two decades with increasing sophistication with our appreciation of intra-abdominal hypertension and abdominal compartment syndrome, the role of complete evacuation of the cytokine-rich intraperitoneal fluid, the need to prevent bowel from adhering to fascia, and the concept of gradual mobilization of fascial edges towards a tension-free closure. Many of these advances are facilitated by increasingly efficient systems that provide negative pressure wound therapy (NPWT) in the open abdomen, such as the ABThera™ Open Abdomen Negative Pressure Therapy System. (Figure 1). Complete details of this system and its application are presented in the ABThera™ Therapy monograph put forth by KCI. Well-designed animal experiments7 have suggested that use of the NPWT may decrease inflammatory response and reduce organ failure,while nonrandomized, multicenter clinical studies document early closure of fascia.
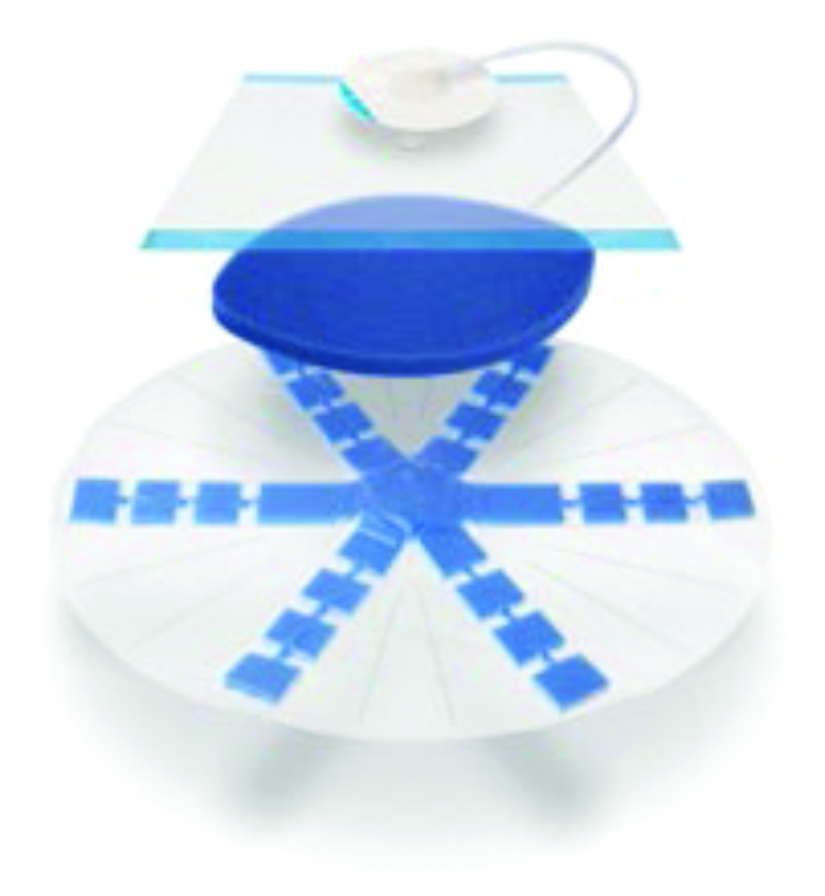 Figure 1. Components of the ABThera™ Open Abdomen Negative Pressure Therapy System
Figure 1. Components of the ABThera™ Open Abdomen Negative Pressure Therapy System
- Nonadherent fenestrated polyurethane visceral protective layer separates the bowel from the abdominal wall, and facilitates the removal of fluid.
- Perforated foam delivers negative pressure, provides medial tension, and minimizes fascial retraction.9
- An occlusive dressing protects the abdominal contents from external contamination
- A SensaT.R.A.C.™ Pad with tubing is placed over the foam and connected to a KCI negative pressure therapy unit.
There are a variety of techniques to use in TAC, and many options are available for fascial closure.10 Mesh-mediated traction, employing a nonabsorbable mesh sutured to the fascial edges and a gradual, sequential tightening to eventual closure is a recently described technique that is very promising with a high rate of fascial closure.
A systematic review8 in 2012 found only two randomized controlled trials and nine cohort studies comparing NPWT and other types of TAC.8 Class I evidence of the superiority of NPWT versus other types of TAC could not be confirmed. Multiple multicenter studies, however, have concluded that NPWT is a viable approach when dealing with critically ill patients being treated by DC procedures.
In summary, the keys to success with open abdomen are exquisite critical care and support of organ function, careful avoidance of iatrogenic injuries to the bowel during dressing changes, avoidance of fluid overload and bowel edema, prevention of enteroatmospheric fistulas, and, most importantly, the closure of open abdomen as early as possible. Success also demands an experienced wound care team that can apply NPWT judiciously to accrue all of its benefits. Continued collaboration between industry and experienced clinician scientists will expand the scope and success of the open abdomen approach in severe sepsis.
References
1. Sartelli M, Catena F, Di Saverio S, et al. Current concept of abdominalsepsis: WSES position paper. World J Emerg Surg. 2014;9:22.
2.Sartelli M, Catena F, Ansaloni L, et al. Complicated intra-abdominal infections in Europe: a comprehensive review of the CIAO study. World J Emerg Surg. 2012;7(1):36.
3.DuBose JJ, Scalea T, Holcomb J, et al. Open abdominal management after damage-control laparotomy for trauma: a prospective observational American Association for the Surgery of Trauma multicenter study. J Trauma Acute Care Surg. 2013;74(1):113-20.
4.Schecter WP, Ivatury RR, Rotondo MF, et al. Open abdomen after trauma and abdominal sepsis: a strategy for management. J Am Coll Surg. 2006;203(3):390-6.
5.Anand RJ, Ivatury RR. Surgical management of intra-abdominal hypertension and abdominal compartment syndrome. Am Surg. 2011;77(Suppl 1):S42-5.
6. Ivatury RR. Update on open abdomen management: achievements and challenges. World J Surg. 2009;33(6):1150-3.
7.Kubiak BD, Albert SP, Gatto LA et al. Peritoneal negative pressure therapy prevents multiple organ injury in a chronic porcine sepsis and ischemia/reperfusion model. Shock 2010;34:525–34.
8.Roberts DJ, Zygun DA, Grendar J, et al. Negative-pressure wound therapy for critically ill adults with open abdominal wounds: a systematic review. J Trauma Acute Care Surg 2012;73(3):629–39.
9.Miller PR, Meredith JW, Johnson JC, Chang MC. Prospective evaluation of vacuum-assisted fascial closure after open abdomen: planned ventral hernia rate is substantially reduced. Ann Surg. 2004;239(5):608-14.
10.Boele van Hensbroek P, Wind J, Dijkgraaf MG et al. Temporary closure of the open abdomen: a systematic review on delayed primary fascial closure in patients with an open abdomen. World J Surg. 2009;33(2):199–207.
11.Acosta S, Bjarnason T, Petersson U, et al. Multicentre prospective study of fascial closure rate after open abdomen with vacuum and mesh-mediated fascial traction. British J Surg. 2011;98(5):735–43.
