
Jeffrey Litt, DO, is an Assistant Professor of Surgery and Medical Director of the Burn and Wound Program at University Hospital’s Frank L. Mitchell Jr., MD, Trauma Center. He joined University of Missouri’s Hugh E. Stephenson Jr., MD, Department of Surgery in July 2014. Born in Iowa but raised in Philadelphia, Dr. Litt completed
undergraduate and medical school in Pennsylvania. He and his wife have two children. Dr. Litt is a consultant for KCI.
Litt_Current Dialogues in Wound Management_2020_Article_15
Negative pressure wound therapy (NPWT) dressings have been a staple in acute and chronic wound management for the last several decades. NPWT dressings have made wound care more manageable and tolerable for patients by decreasing the frequency of dressing changes-often 2-3 times weekly depending on the wound type, size, and exudate, as opposed to once or twice a day. NPWT dressings have also been shown to accelerate healing by creating an environment that promotes wound healing through biomechanical and cellular forces on the wound bed and surrounding tissues.1 Recently, NPWT has evolved to include the addition of instillation of a topical wound solution (V.A.C. VERAFLO™ Therapy). This instillation assists with more frequent wound bed lavage and biomechanical stretch, and compression of the wound bed has been shown to accelerate debris removal and improved granulation tissue formation.2 The V.A.C. VERAFLO CLEANSE CHOICETM Dressing was developed for use with V.A.C. VERAFLO™ Therapy specifically for wounds with thick exudate and to facilitate wound cleansing.
In the burn care arena, NPWT dressing utilization is likewise well documented. Of all of the potential applications of negative pressure utilization in burn patients, usage as a split-thickness skin graft (STSG) bolster is the most common and the use that boasts the most peer-reviewed data.3;4 Still, usage as a primary dressing modality for acute burns has been researched and published.5;6 Being a relatively new technological advancement to the wound care treatment armamentarium, less research is available discussing the use of V.A.C. VERAFLO™ Therapy with V.A.C. VERAFLO CLEANSE CHOICE™ Dressing in this area. A recent article and case review from the burn group at the Arizona Burn Center concluded that usage of V.A.C. VERAFLO CLEANSE CHOICE™ Dressing, especially with a hypochlorous acid instillation solution, resulted in a shorter time to wound closure with skin grafting in a burn or necrotizing soft tissue infection population.7 Experience utilizing this technology in burn care is growing. We discuss two recent cases that underwent burn/thermal injury wound care to assist in the management of ultimate closure of their wounds.
Case 1
A 55-year-old male was found in his home, unresponsive and hypothermic during an especially frigid spell in January. The patient was intubated prior to arrival with suspected pressure wounds. After active rewarming and resuscitation, the patient’s wounds were better addressed, and consisted of wounds to both forefeet and heels consistent with stage 4 frostbite as well as wounds to his right hand and arm consistent with full-thickness contact burns from being found unresponsive on his space heater (Figures 1-2). It is important to note that V.A.C. VERAFLO™ Therapy is not indicated for use on full-thickness burns.


Ultimately, once the patient stabilized, the burn team brought him to the operating room for initial excision of his arm and hand burns. The patient was observed to have poorly controlled, Type 1 diabetes with a history of coronary artery disease. At this initial operation, his right hand was noted to be severely burned with exposed and damaged tendon and bones on his 4 fingers (Figure 3).

The patient had full-thickness burns to his forearm and arm, as well. Ultimately, he underwent amputation of his lateral 3 fingers and autografting of his arm wounds. His remaining hand was managed with a groin flap, and he ultimately retained his thumb and forefinger (Figure 4).

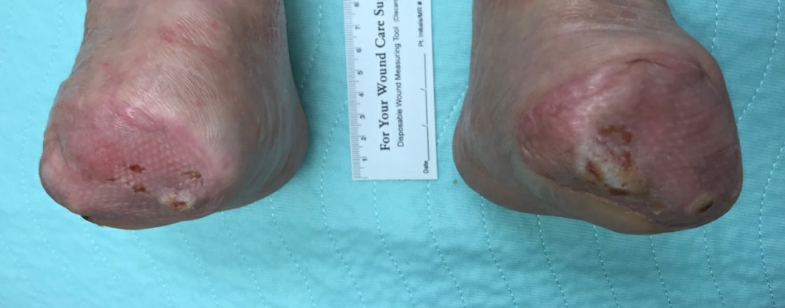
The patient’s feet were managed conservatively to allow for wound demarcation, consistent with standard frostbite management. He continued to improve clinically and ultimately was extubated without signs of anoxic brain injury. Approximately 6 months after his initial injury his foot wounds demarcated to the point of requiring more definitive closure (Figures 5-6).


In an attempt to preserve his feet and legs and avoid bilateral below-knee amputations, transmetatarsal amputations were performed, with staged closure using a dermal template and eventual split-thickness skin graft application. The patient also received bilateral full-thickness skin grafts to his heels at this time. Post-amputation, V.A.C. VERAFLO™ Therapy using a V.A.C. VERAFLO CLEANSE CHOICE™ Dressing was utilized to accelerate wound bed preparation. Normal saline (30 mL right, 20 mL left) was instilled into the wound bed with a dwell time of 3 minutes, followed by 2 hours of negative pressure at -125 mmHg. Dressing changes occurred every 2-3 days. Excellent wound bed preparation was achieved with full wound bed coverage with healthy granulation tissue following V.A.C. VERAFLO™ Therapy with V.A.C. VERAFLO CLEANSE CHOICE™ Dressing use after 7 days (Figure 7). Ultimately the patient was approved for skin grafting after staging with neo-dermis (Kerecis® Omega3 Wound Acellular Dermal Matrix, Kerecis LTD, Arlington, VA) to help with deeper tissue coverage. Approximately two weeks later, the patient’s bilateral foot wounds were optimized, and he received STSG with NPWT bolstering, which resulted in excellent (100%) graft take. The patient is currently ambulatory at home, able to wear offloading boots, and is being fitted for forefoot orthotics to assist with his balance over his well-healed and stable skin grafts (Figure 8).

Case 2
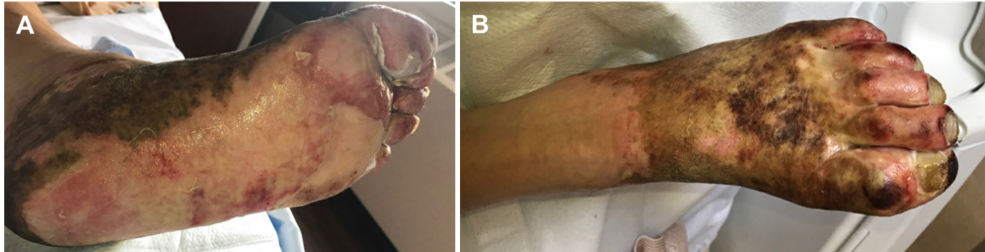
A 60-year-old male with numerous comorbidities including severe aortic stenosis as well as uncontrolled diabetes and resultant neuropathies resulting in a prior above-the-knee amputation of his right leg presented for care. The patient sustained a chemical burn with bleach on his left foot the day prior to admission to our facility and was transferred to our center from an outside facility after decontamination occurred with a presumptive diagnosis of sepsis from this extensive left foot wound. In the emergency room, non-excisional debridement of his foot occurred, and local wound care was performed after admission to the hospital with appropriate antibiotics as he stabilized. The patient’s entire foot was involved, with full-thickness wounds noted throughout (Figures 9).
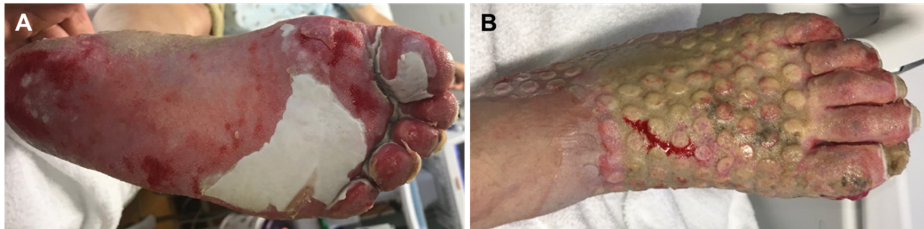
The patient was felt to be a poor surgical candidate for standard operative excisional debridement, and he refused to discuss the possibility of a second leg amputation under regional anesthesia. Given the need for further wound cleansing and debris removal, we utilized V.A.C. VERAFLO™ Therapy with V.A.C. VERAFLO CLEANSE CHOICE™ Dressing on hospital day 2 with 50 mL of normal saline for instillation, a dwell time of 5 minutes, followed by 2 hours of negative pressure at -125 mmHg. Dressings were changed every 2-3 days. At dressing removal, approximately 50% of the eschar had separated and the wounds were improving (Figure 10). The V.A.C. VERAFLO™ Therapy was discontinued on hospital day 6 to allow for discharge to home with a silver-impregnated foam.
The patient was seen in clinic approximately 2 weeks later, with continued healing and silver dressings applied. We continued bi-weekly outpatient visits for approximately the next 6 weeks, and his foot was nearly 100% healed and epithelialized 3 months following his initial injury (Figure 11).

While NPWT dressings are commonly used in wound care and burn care, the use of V.A.C. VERAFLO ™ Therapy with V.A.C. VERAFLO CLEANSE CHOICE™ Dressing being used for acute burns and traumatic or infected wound management is slowly increasing in usage. One of the reasons why it is being slowly adopted is that many practitioners are unfamiliar with the technology, the appropriate instillation solution, and the settings required to maximize patient outcomes. In our academic medical center, both in burns as well as other wound etiologies, the experience of using the V.A.C. VERAFLO ™ Therapy with V.A.C. VERAFLO CLEANSE CHOICE™ Dressing was likewise slowly adopted until our comfort level improved; not only with application of the dressings and technology, but likewise with understanding of the clinical rationale behind using certain settings and/or topical wound solution use in specific scenarios-with much of this information being gained through the direct experience of using the V.A.C. VERAFLO™ Therapy. While reviews of the evidence and clinical practice guidelines have been published and are very useful,8-10 we have found that the practical experience of “just doing it”, (i.e. using the V.A.C. VERAFLO™ Therapy in different clinical scenarios to understand its place in the wound healing algorithm) ultimately informed our usage even more than the peer-reviewed literature. Recently, an update to the international consensus guidelines was published detailing appropriate wound types, topical wound solution types, and appropriate starting settings, such as amount of negative pressure and the optimal dwell/suction time(s).10 Inexperienced practitioners looking to begin initiating the V.A.C. VERAFLO™ Therapy for burns, or other various wounds, should look to these and other practice guidelines for starting points. The experience of using the technology allows for the customization based on wound and patient specifics; but the “starting settings” are most frequently sufficient for most wounds on most patients to help promote wound healing.
The use of V.A.C. VERAFLO™ Therapy with V.A.C. VERAFLO CLEANSE CHOICE™ Dressing in burn care has great potential to act as the primary wound dressing for burns that need staging and may help prevent burn wound progression in mixed-depth or deeper burns. In my experience, V.A.C. VERAFLO™ Therapy also has a role in the reconstruction of burn or thermal injury wounds by helping optimize the wound bed. In our experience, its usage, especially in the medically frail, complex patient, or burn wound can be helpful in wound cleansing.
Patient data and photos courtesy of Jeffrey Litt, DO.
As with any case study, the results and outcomes should not be interpreted as a guarantee or warranty of similar results. Individual results may vary depending on the patient’s circumstances and condition.
NOTE: Specific indications, contraindications, warnings, precautions, and safety information exist for these products and therapies. Please consult a clinician and product instructions for use prior to application. Rx only.
References
Saxena V, Hwang CW, Huang S, Eichbaum Q, Ingber D, Orgill DP. Vacuum-assisted closure: microdeformations of wounds and cell proliferation. Plast Reconstr Surg 2004;114(5):1086-1096.
Kim PJ, Attinger CE, Steinberg JS et al. The impact of negative-pressure wound therapy with instillation compared with standard negative-pressure wound therapy: a retrospective, historical, cohort, controlled study. Plast Reconstr Surg 2014;133(3):709-716.
Scherer LA, Shiver S, Chang M, Meredith JW, Owings JT. The vacuum assisted closure device: a method of securing skin grafts and improving graft survival. Arch Surg 2002;137(8):930-934.
Llanos S, Danilla S, Barraza C et al. Effectiveness of negative pressure closure in the integration of split thickness skin grafts: a randomized, double-masked, controlled trial. Ann Surg 2006;244(5):700-705.
Chong SJ, Liang WH, Tan BK. Use of multiple VAC devices in the management of extensive burns: the total body wrap concept. Burns 2010;36(7):e127-e129.
Kantak NA, Mistry R, Varon DE, Halvorson EG. Negative Pressure Wound Therapy for Burns. Clin Plast Surg 2017;44(3):671-677.
Matthews MR, Hechtman A, Quan AN, Foster KN, Fernandez LG. The Use of V.A.C. VERAFLO CLEANSE CHOICE in the Burn Population. Cureus 2018;10(11):e3632.
Kim PJ, Attinger CE, Crist BD et al. Negative pressure wound therapy with instillation: review of evidence and recommendations. Wounds 2015;27(12):S2-S19.
McKanna M, Geraci J, Hall K et al. Clinician panel recommendations for use of negative pressure wound therapy with instillation. Ostomy Wound Manage 2016;(Suppl):3-14.
Kim PJ, Attinger CE, Constantine T et al. Negative pressure wound therapy with instillation: International consensus guidelines update. Int Wound J 2020;17(1):174-186.
©Copyright 2020 3M. All rights reserved. 3M and the other marks shown are marks and/or registered marks. Unauthorized use prohibited. PRA-PM-US-02532 (06/20).
