
Jeffrey Litt, DO, is an Assistant Professor of Surgery and Medical Director of the Burn and Wound Program at University Hospital’s Frank L. Mitchell Jr., MD, Trauma Center. He joined MU’s Hugh E. Stephenson Jr., MD, Department of Surgery in July 2014. Born in Iowa but raised in Philadelphia, Dr. Litt completed undergraduate and medical school in Pennsylvania. He and his wife have two children.
Litt_Current Dialogues in Wound Management_2017_Volume 3_Issue 1
NOTE: As with any case study, the results and outcomes should not be interpreted as a guarantee or warranty of similar results. Individual results may vary depending on the patient’s circumstances and condition.
The incidence of acute traumatic wounds in the United States is substantial; of 136+ million emergency department visits in 2011, 30+ million were related to ICD-9 codes related to “injuries”, with 11+ million related to open or closed wounds or burns1. Potentially the most horrifying of these traumatic wounds are the major, degloving-type soft tissue injuries. No tracking is available for evaluating the incidence or the outcomes of these particular wounds, and their early care is frequently complicated by injury severity and presence of concomitant and often life-threatening separate injuries. Nonetheless, early recognition of these injuries, in particular the closed space, “internal degloving” injuries, such as Morel-Lavallée lesions (MLL) impacts long-term morbidity and even mortality. When these injured patients present to the trauma center care frequently involves multidisciplinary teams for optimizing outcomes. A brief review of the evaluation and subsequent care of patients with these injuries will be discussed, followed by a brief case report of a recently injured patient at our level 1 trauma center describing how the multidisciplinary care of a severely injured patient enhanced his recovery to the point of eventual discharge to home.
 Figure 1. The 18-inch drainpipe our patient was swept through. Note – this pipe was entirely underwater and only reachable by boat at the time of the incident.
Figure 1. The 18-inch drainpipe our patient was swept through. Note – this pipe was entirely underwater and only reachable by boat at the time of the incident.
Degloving-type soft-tissue injuries are an avulsion-type injury of the skin and subcutaneous tissues. In these injuries, portions of the subcutaneous tissues, as well as the overlying skin components detach partially or completely from their underlying tissue attachments. These injuries most commonly occur in the limbs, but can occur on the scalp, trunk, or pelvis. Associated severe accompanying injuries and substantial blood loss can occur, and so frequently all or a portion of the avulsed structures are non-viable and lost. Early recognition is key. Open soft-tissue avulsions are clearly easily recognized, if not always easily treated. Early treatment consists primarily of hemorrhage control, removal of visible non-viable tissues, and local wound care until definitive repair or closure can occur. This can potentially be done in an immediate fashion in the stable patient, but more frequently occurs in a staged fashion in the severely injured patient. Closed avulsion injuries, on the other hand are more difficult to identify, and their potential complication risk can be as high if not higher than similar open injuries secondary to delays in appropriate treatment and resultant infection, sepsis, tissue loss, or even death.
 Figure 2. The patients entirely degloved right chest wall HD2 s/p; note tube thoracostomy.
Figure 2. The patients entirely degloved right chest wall HD2 s/p; note tube thoracostomy.
Classification of these injuries is based on 4 potential patterns of injury, with prognosis and treatment being affected by the pattern. Arnez, et al. evaluated 68 patients with 79 openly injured limbs2. Evaluating injury patterns and subsequent healing they concluded a general evaluation and treatment algorithm, namely;
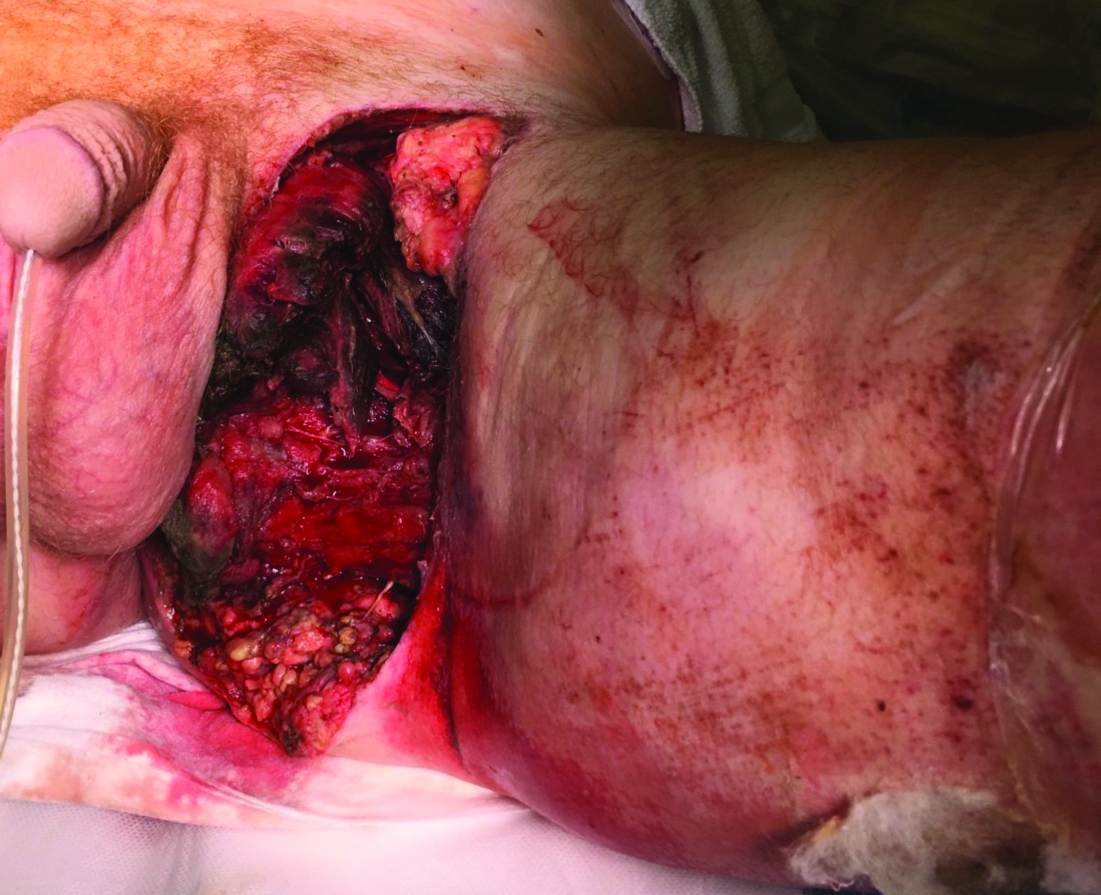 Figure 3. Left groin degloving; femoral triangle structures were grossly exposed (not visible in this photograph). Also note proximity to left anus.
Figure 3. Left groin degloving; femoral triangle structures were grossly exposed (not visible in this photograph). Also note proximity to left anus.
Pattern 1 – Limited degloving with abrasion/avulsion – often occur over bony prominences and free tissue transfer often needed due to exposure of underlying tendon/joint/bony tissues.
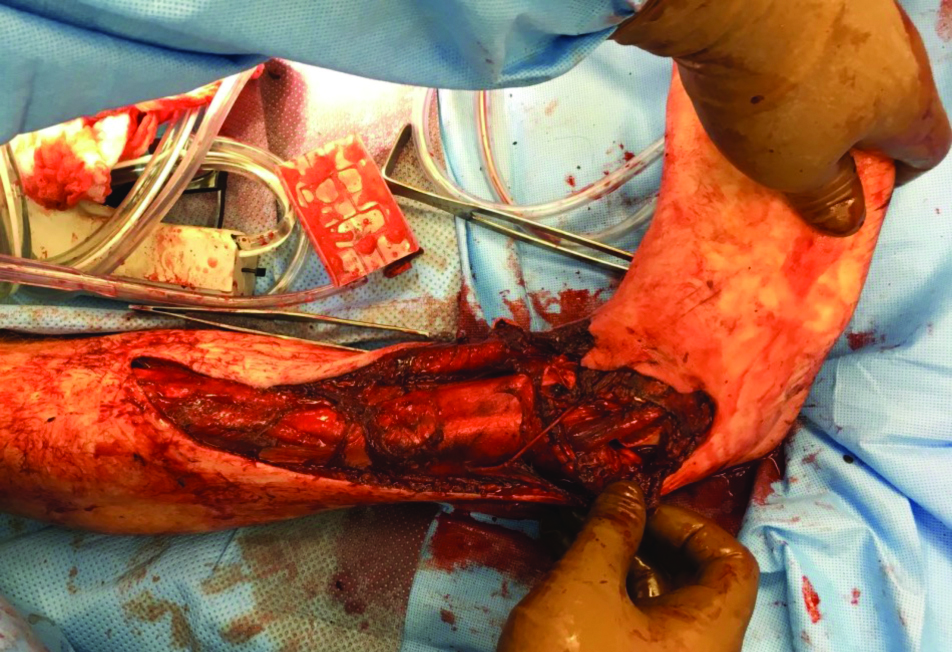 Figure 4. Right lower extremity degloving injury with exposed tibia and open (contaminated) ankle joint.
Figure 4. Right lower extremity degloving injury with exposed tibia and open (contaminated) ankle joint.
Pattern 2 – Non-circumferential degloving injury – avulsion plane typically confined to a single layer. Careful flap evaluation, possibly with assistance of perfusion technology (i.e. fluorescein, indocyanine green fluoroscopic evaluation, etc.) may delineate perfusion of tissue flap and allow for primary closure.
Pattern 3 – Circumferential single plane degloving – similar to Pattern 2 but with significantly more soft tissue involvement; operative debridement usually necessary with secondary operative procedures, i.e. split-thickness skin grafting or full-thickness transfer flaps.
 Figure 5. Patients R hand 1 week post-operatively from reverse radial flap (note skin graft to donor site proximally).
Figure 5. Patients R hand 1 week post-operatively from reverse radial flap (note skin graft to donor site proximally).
Pattern 4 – Circumferential multi-planar degloving – greatest amount of tissue damage is present. Staged reconstruction is likely required
In addition, degloving-type injuries can occur in an open or closed fashion.
The previously described patterns describe open injuries. Morel-Lavallée lesions (MLL), first described by French physician Maurice Morel- Lavallée in 1863, specifically describe closed hemolymphatic collections developing from severe soft tissue injuries to the thigh. They occur most commonly in motor-vehicle accidents, but can occur from any crushing or shearing-type injury. They and similar MLL-type injuries occur primarily in the trunk or lower extremities, and are associated with pelvic trauma or thigh injuries a majority of the time3. A review of the literature by Vanhegan et al. identified 204 lesions from 29 articles, with a breakdown by site of incidence as follows: greater trochanter/hip, 30.4 %; thigh, 20.1 %; pelvis, 18.6 %; knee, 15.7 %; gluteal, 6.4 %; lumbosacral, 3.4 %; abdominal, 1.5 %; calf/lower leg, 1.5 %; head, 0.5 %; and not specified, 2.0 %4. They are shear-type injuries, where force applied against the skin and superficial tissues causes movement of the relatively mobile skin and subcutaneous tissues over the relatively immobile underlying deeper fascial tissues, causing disruption and shearing of vascular structures and resultant hemolymphatic fluid collection. If not identified early, potential infection, overlying skin necrosis, and even necrotizing infection, sepsis, or death may occur.
 Figure 6. Right lower extremity latissimus dorsi flap and skin graft, approximately 2 months after initial injury (and 1 month after surgery).
Figure 6. Right lower extremity latissimus dorsi flap and skin graft, approximately 2 months after initial injury (and 1 month after surgery).
 Figure 7. Left groin wound, nearly completely healed at same visit.
Figure 7. Left groin wound, nearly completely healed at same visit.
Closed degloving injuries are frequently identified early after presentation in the multiply-injured major trauma patient. In the patient with more minor injuries, the MLL-type lesions may present more insidiously and may take days, or rarely even years to be properly identified. Like most medical events, a classification system has been developed with regards to chronicity and imaging characteristics. These classifications progress in chronicity, with a Type 1 lesion being an acute hematoma/seroma, and a Type 6 lesion describing an infected chronic encapsulated lesion. Type of lesions, however, is not especially related to prognosis or treatment, unlike open degloving injuries. Imaging can be accomplished with nearly any modality, but MRI is imaging modality of choice, particularly in patients with potential sub-acute or chronic lesions
Management of these lesions partially depends on the chronicity of the lesion. Options include compression, percutaneous aspiration (frequently under imaging guidance), open drainage, cavity lavage, and even sclerosis of the cavity/capsule for long-standing lesions. Dawre et al. in 2012 proposed treatment algorithms for both acute and chronic lesions5. They recommend, when possible, an initial attempt at conservative management or percutaneous drainage, +/- sclerosis prior to attempting open drainage5. Occasionally, however, late-diagnosed patients present in sepsis from their lesions, requiring open drainage along with frequent skin and subcutaneous tissue debridement and staged reconstruction, most frequently with split-thickness skin grafting, although usage of avulsed flap skin as a full-thickness skin graft has been utilized in limited case series.
Regardless of whether a degloving injury is open or closed, these are extremely serious injuries, and when patients are victims of polytrauma, may require multidisciplinary approaches to care. We present the case of a 33 year old male farmer for whom we recently cared who, along with 2 friends, presented as a polytrauma victim after being sucked through an 18 inch drainpipe (see Fig 1) during heavy flooding on his farm in a drainage pond.
He was brought in as a level 1 alert, having suffered multiple soft-tissue injuries as well as significant orthopedic injuries to all 4 extremities and his left groin as well as his right chest wall, with exposed underlying structures at all sites (Fig 2-4).
Initial evaluation was per ATLS standards, and Orthopedics was present on initial evaluation. The initial list of injuries is too lengthy to list here, but most significantly, the patient sustained right second MCP open arthrotomy, right elbow traumatic arthrotomy, right ankle arthrotomy, left hip traumatic arthrotomy, large soft tissue defects in the right upper, right lower, and left lower extremities as well as right chest wall soft tissue defect with exposed ribs and open chest wound. Significant pond-water and debris contamination was noted throughout all of the wounds. Initial sharp debridement and wound irrigation occurred in of all of his soft-tissue injuries. Orthopedics evaluated his wounds (V.A.C.® Therapy System and V.A.C.® GRANUFOAM SILVER™ Dressings), and after stabilization in the SICU, in conjunction with our trauma/acute care surgery team, serial debridements of all soft tissue and joint-involvement wounds occurred during hospitals days (HD) 1-5. Negative-pressure dressings were used for his chest wall wound and right upper and lower extremity wounds, with Dakins-soaked gauze utilized in his left groin wound. At this point Plastic Surgery was consulted for assistance with closure of his large left groin wound, measuring approximately 15 x 15 x 2 cm. Exposed femoral neurovascular structures were noted on their exam, without significant neurovascular injury, and operative coverage plan of a pedicled flap was made. The patient did receive a diverting colostomy for perianal wound care purposes on HD10. On HD16 Plastic Surgery performed a left groin debridement, antibiotic bead placement, and pedicled rectus abdominis flap with negative pressure dressing (V.A.C.® Therapy System and V.A.C.® GRANUFOAM SILVER™ Dressings). Simultaneous with this procedure, Orthopedic Hand Surgery performed a reverse radial forearm flap for right hand coverage (Fig 5).
The patient recovered from these procedures and underwent serial negative-pressure dressing changes over the next 12 days, after which he underwent a free latissimus dorsi flap with split-thickness skin graft to the right ankle with the Orthopedic Surgery service. Over the next 2 weeks the patient underwent split-thickness skin grafts to his chest wall, his bilateral lower extremities, and revision of his left groin using negative pressure as a bolster by the trauma/burn as well as Plastics teams, with primarily excellent healing and skin-graft take on all of these wounds. He was discharged to inpatient
rehabilitation on HD 54. His wounds have all closed and healed (Fig 6-7).He has since been readmitted and underwent a left total hip replacement for left hip contracture and heterotopic ossification of the left hip, and was subsequently discharged to home, 3 months exactly after his initial injury. While he is still undergoing intensive home therapy, he survived horrific injuries and, after more than 2 dozen surgeries and procedures, is weight-bearing and ambulatory, and importantly has all 4 of his limbs. Plans for ostomy reversal are pending. Multidisciplinary surgical care was an absolute requirement for his care and outcome optimization, in in this case, was extremely effective.
References
1.National Hospital Ambulatory Medical Care Survey: 2011 Emergency Department Summary Tables. Hyattsville, MD: National Center for Health Statistics, 2012.
2.Arnez, ZA. Khan, U. Tyler, MPH., Classification of Soft-Tissue Degloving in Limb Trauma. Journal of Plastic, Reconstructive, and Aesthetic Surgery. (2010);63:1865-69
3.Latifi, R. El-Hennawy, H. et al. The Therapeutic Challenges of Degloving Soft-Tissue Injuries. J Emerg Trauma Shock. (2014);7(3):228-32
4.Bonilla-Yoon, I. Masih, S, et al. The Morel-Lavallée Lesion: Pathophysiology, Clinical Presentation, Imaging Features, and Treatment Options. Emerg Radiol. (2014);21:35-43
5.Dawre, S. Lamba, S. et al. The Morel-Lavallée Lesion: A Review and a Proposed Algorithmic Approach. Eur J Plast Surg. (2012);35:489-94
