
Marcus S. Speyrer, RN, CWS is the Chief Operating Officer and Partner in The Wound Treatment Center, LLC @ Opelousas General Health System in Opelousas, LA. He began in wound care in 1993. He is a Registered Nurse and Certified Wound Specialist. He received his Associate Degree in Nursing at the University of New York-Regents College in 1995.
Speyrer_Current Dialogues in Wound Management_2017_Volume 3_Issue 2
NOTE: As with any case study, the results and outcomes should not be interpreted as a guarantee or warranty of similar results. Individual results may vary depending on the patient’s circumstances and condition.
INTRODUCTION
Wound care centers (WCCs) were developed to meet the need of providing wound care to increasing numbers of patients with acute, postsurgical, and chronic wounds. Our WCC sees a multitude of complex patients, who have often failed previous wound care treatments. Our wound care plan typically includes the use of debridement and several advanced modalities such V.A.C.® Therapy and cellular and/or tissue based products. However, in recent years, this plan has been difficult to follow due to changes in reimbursement policies. In 2014, the Centers for Medicare and Medicaid Services (CMS) implemented the bundle payment system for all cellular and/or tissue based products. Once enacted, it became increasingly challenging to prescribe this therapy for our patients as it caused reimbursement of cellular and/or tissue based products at a rate lower than the cost of the product for our WCC. Without availability of these products, we needed another option in providing wound management for our patients with chronic wounds.
ADDITION OF NEW TOOLS TO OUR WOUND CARE TREATMENT PLAN
For a subset of patients, wound closure is not possible without the application of cellular and/or tissue based products; however, the use of these products has become cost prohibitive. In examining our available therapy options, we identified the combination of PROMOGRAN PRISMA™ Matrix for wound bed preparation, followed by epidermal grafting as an advanced wound care plan that might promote would healing in our patients.
PROMOGRAN PRISMA™ Matrix is an advanced wound dressing comprised of a sterile, freeze dried composite of 44% oxidized regenerated cellulose (ORC), 55% collagen, and 1% silver-ORC. This dressing is different from other silver dressings, as the silver is ionic and the use of sterile saline to pre-moisten the dressing does not alter its silver properties. We had previously observed positive clinical results with the use of PROMOGRAN PRISMA™ Matrix in our patients. Therefore, we believed that this dressing could potentially optimize wounds for epidermal grafting by promoting healthy granulation tissue formation.
In recent years, epidermal grafting has been shown to be a viable alternative to traditional skin grafting.1,2 Here, only the epidermal layer, which is harvested into small microdomes is applied to the wound in order to promote wound closure. In our center, the CELLUTOME™ Epidermal Harvesting System has been used to reproducibly harvest uniform epidermal microdomes. The harvester is placed on patient’s thigh and connected to the CELLUTOME™ System vacuum head. Negative pressure and heat are applied to the donor site to raise epidermal microdomes, which are then harvested and transferred to the wound. Epidermal grafting has been previously used in our patients, resulting in wound area reduction and/or wound closure.
The use of PROMOGRAN PRISMA™ Matrix or epidermal grafting in our patients has promoted wound healing. As both advanced wound therapies offered positive results, we used both in the care of a handful of patients. Complete wound re-epithelialization has been observed in our patients following the treatment with PROMOGRAN PRISMA™ Matrix in conjunction with epidermal grafting. With these positive clinical results, we updated our existing wound care pathway to include the use of PROMOGRAN PRISMA™ Matrix, followed by epidermal grafting.
REPRESENTATIVE CASE STUDY
A 40-year-old male truck driver was referred to us for care following a lower extremity fasciotomy secondary to deep vein thrombosis (Figure 1A). Previous medical history included diabetes mellitus and tobacco abuse (smoker). The patient underwent surgical debridement followed by V.A.C.® Therapy at -125mmHg and hyperbaric oxygen therapy at 2.0 atmosphere absolute for 90 minutes for a total of 21 days of V.A.C.® Therapy (Figure 1B). Within those 21 days, the patient underwent two additional surgical debridements, as well as a total of 27 hyperbaric treatments, during which V.A.C.® Therapy was temporarily interrupted and reapplied, per the manufacturer’s instructions for use and warnings. V.A.C.® Therapy was then discontinued, and PROMOGRAN PRISMA™ Matrix was applied to his wound every other day for five weeks until the wound was ready for epidermal grafting (Figure 1C). On the day of epidermal grafting, the patient’s right thigh was prepped by removing hair and the skin cleansed with isopropyl alcohol. Epidermal microdomes formed within 20 minutes and were transferred to the wound using a silver foam dressing (Mepilex® Ag, Mölnlycke Health Care, Norcross, GA). The dressing was secured with a self-adherent wrap and an elastic bandage while the donor site was covered with a foam dressing (Mepilex® Border, Mölnlycke Health Care). The patient tolerated the procedure well without any pain or discomfort. At 7 days post grafting (Figure 1D), the dressing was removed, and PROMOGRAN PRISMA™ Matrix was applied. The donor site was also completely healed without complications. We continued to apply PROMOGRAN PRISMA™ Matrix every other day to the wound for 15 weeks (Figure 1E). After 15 weeks, the patient was discharged from the WCC with an almost completely healed wound. He returned to work without any restrictions or complications.
DISCUSSION
Our WCC manages patients with complex comorbidities and wounds that, oftentimes, have failed previous wound care treatments. Prior to the CMS reimbursement change, we used debridement, V.A.C.® Therapy, and cellular and/or tissue based products to facilitate wound closure. Once it became cost prohibitive to use cellular and/or tissue based products, we added PROMOGRAN PRISMA™ Matrix for wound bed preparation, followed by epidermal grafting to our existing wound care management plan.
PROMOGRAN PRISMA™ Matrix helps maintain a moist wound environment, which is conducive to granulation tissue formation, re-epithelialization, and wound healing.3,4Following wound bed preparation with PROMOGRAN PRISMA™ Matrix, epidermal grafting using microdomes harvested with the CELLUTOME™ System are utilized. With this system, we are able to obtain reproducible epidermal microdomes in the outpatient or office setting with no anesthesia required and minimal pain and donor-site trauma.5,6 At our WCC, the combination of PROMOGRAN PRISMA™ Matrix followed by epidermal grafts harvested with the CELLUTOME™ System has become an integral part of our armamentarium in dealing with chronic wound management.
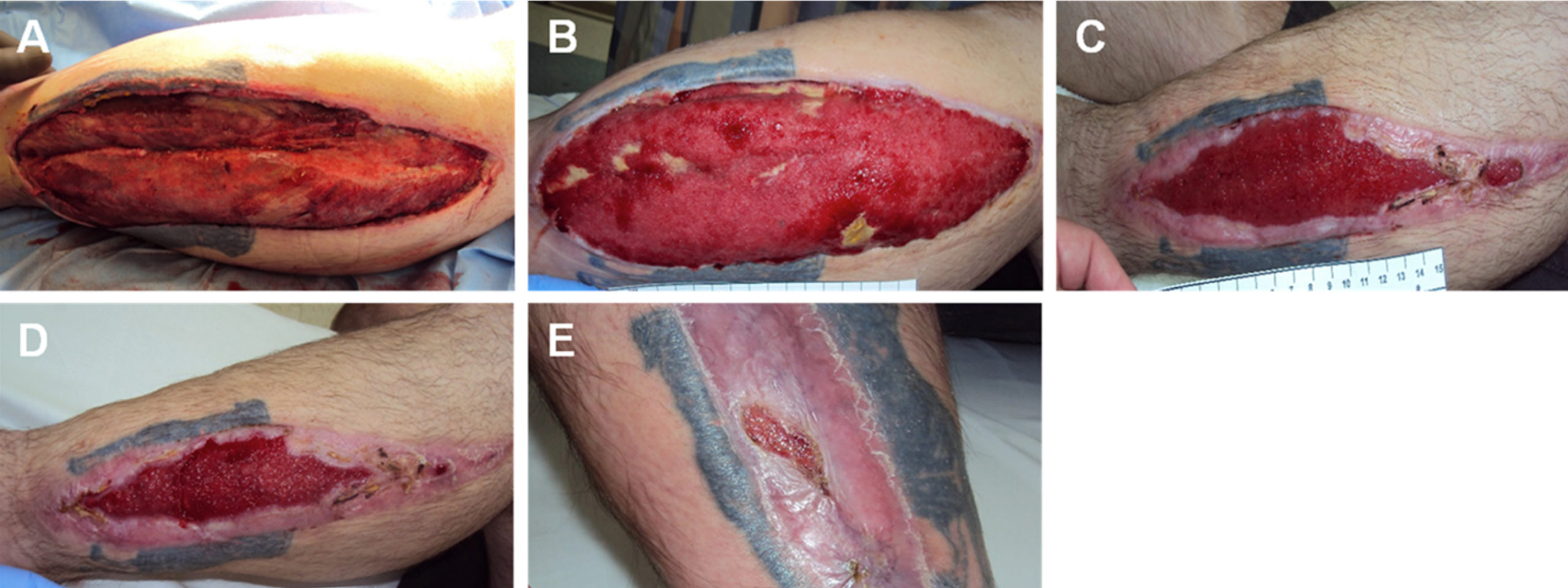 Figure 1: Wound following lower leg fasciotomy. A. Wound at presentation to the wound care center; B. Wound after 27 hyperbaric oxygen therapy treatments and 21 days of V.A.C.® Therapy; C. Wound on day of epidermal grafting, following 5 weeks of PROMOGRAN PRISMA™ Matrix; D. Wound 7 days post grafting; E. Wound after 15 weeks of PROMOGRAN PRISMA™ Matrix.
Figure 1: Wound following lower leg fasciotomy. A. Wound at presentation to the wound care center; B. Wound after 27 hyperbaric oxygen therapy treatments and 21 days of V.A.C.® Therapy; C. Wound on day of epidermal grafting, following 5 weeks of PROMOGRAN PRISMA™ Matrix; D. Wound 7 days post grafting; E. Wound after 15 weeks of PROMOGRAN PRISMA™ Matrix.
References
1.Richmond NA, Lamel SA, Braun LR, Vivas AC, Serena T, Kirsner RS. Epidermal grafting using a novel suction blister-harvesting system for the treatment of pyoderma gangrenosum. JAMA Dermatology2014;150:999-1000.
2.Lincoln K, Hyde J. Evaluation of epidermal skin grafts for the treatment of complex wounds in a wound care center: A 94-patient case series. Wounds 2016;28:347-353.
3.Gottrup F, Cullen BM, Karlsmark T, Bischoff-Mikkelsen M, Nisbet L, Gibson MC. Randomized controlled trial on collagen/oxidized regenerated cellulose/silver treatment. Wound Repair Regen2013;21:216-225. doi:10.1111/wrr.12020.
4.Cullen B, Watt PW, Lundqvist C et al. The role of oxidised regenerated cellulose/collagen in chronic wound repair and its potential mechanism of action. Int J Biochem Cell Biol 2002;34:1544-1556.
5.Osborne SN, Schmidt MA, Harper JR. An Automated and Minimally Invasive Tool for Generating Autologous Viable Epidermal Micrografts. Adv Skin Wound Care 2016;29:57-64. doi:10.1097/01.ASW.0000476072.88818.aa.
6.Osborne SN, Schmidt MA, Derrick K, Harper JR. Epidermal micrografts produced via an automated and minimally invasive tool form at the dermal/epidermal junction and contain proliferative cells that secrete wound healing growth factors. Adv Skin Wound Care 2015;28:397-405.
